


Intelligent Healthcare Ecosystems: An Essential Guide
The numbers tell you why this topic matters now. The global AI in healthcare market was valued at $36.7 billion in 2025 and is projected to reach $505.6 billion by 2033, with a projected CAGR of 38.9%, according to Grand View Research's healthcare AI market outlook. That scale of projected investment says something important. Healthcare organizations aren't buying another dashboard. They're trying to redesign how care, operations, and data work together.
An intelligent healthcare ecosystem isn't a product category. It's an operating model. Patients, clinicians, administrators, payers, devices, and software systems exchange data in ways that let the organization act earlier, coordinate better, and learn continuously. That sounds ambitious because it is.
What usually gets lost in the hype is the prerequisite. A smarter ecosystem doesn't start with AI features. It starts with trustworthy data, disciplined governance, and architecture that can support real-world care delivery without breaking privacy, compliance, or clinician workflow. If you're trying to build products in this space, that's the difference between a polished demo and a durable platform.
The Dawn of Connected Proactive Healthcare
Healthcare used to be organized around isolated encounters. A patient showed up. A clinician diagnosed. A hospital treated. Another system handled billing. A separate app handled follow-up, if there was follow-up at all. Most organizations still carry traces of that design.
An intelligent healthcare ecosystem changes the underlying logic. Instead of reacting to episodes, it connects signals across the care journey so teams can anticipate need, guide decisions, and reduce avoidable friction. The practical shift is from siloed systems to coordinated workflows.
What the ecosystem actually is
Think of it as a network, not a suite. The network includes:
-
Patients using portals, telehealth tools, wearables, remote monitoring devices, and care management apps
-
Providers working across EHRs, imaging systems, triage tools, scheduling platforms, and decision support
-
Payers and operations teams managing claims, authorizations, compliance checks, and financial workflows
-
Data and AI services that connect these moving parts and turn raw activity into recommendations or automation
That's why many organizations underestimate the challenge. They budget for features and discover they need interoperability, identity resolution, governance rules, model monitoring, and workflow redesign.
Why this shift is different
The current push isn't only about digitizing healthcare. It's about making digital systems collaborate. A scheduling tool on its own doesn't create intelligence. A claims engine on its own doesn't create intelligence. A predictive model on its own certainly doesn't. The ecosystem becomes intelligent when each part contributes to a shared operating picture.
Practical rule: If the data can't move cleanly between clinical, operational, and patient-facing systems, the ecosystem won't behave intelligently no matter how advanced the model is.
This is also why product leaders need to think beyond isolated use cases. A remote monitoring app may look successful in pilot mode, but if it can't feed clinicians actionable context inside daily workflows, adoption stalls. The same applies to AI copilots, patient engagement tools, and automation platforms.
For teams building platforms in this category, the bar is higher than feature delivery. You need systems thinking. You need governance. And if you want to grow into a credible healthtech software development partner, you need to understand that the ecosystem is the product.
The Core Components of an Intelligent Ecosystem
A useful way to understand intelligent healthcare ecosystems is to stop thinking in terms of apps and start thinking in layers. A mature system integrates Data Connectivity, Intelligence, Automation, Experience, and Governance/Ethics, and this layered model can reduce resource misallocation by up to 30%, as described in Globant's analysis of predictive health ecosystems.
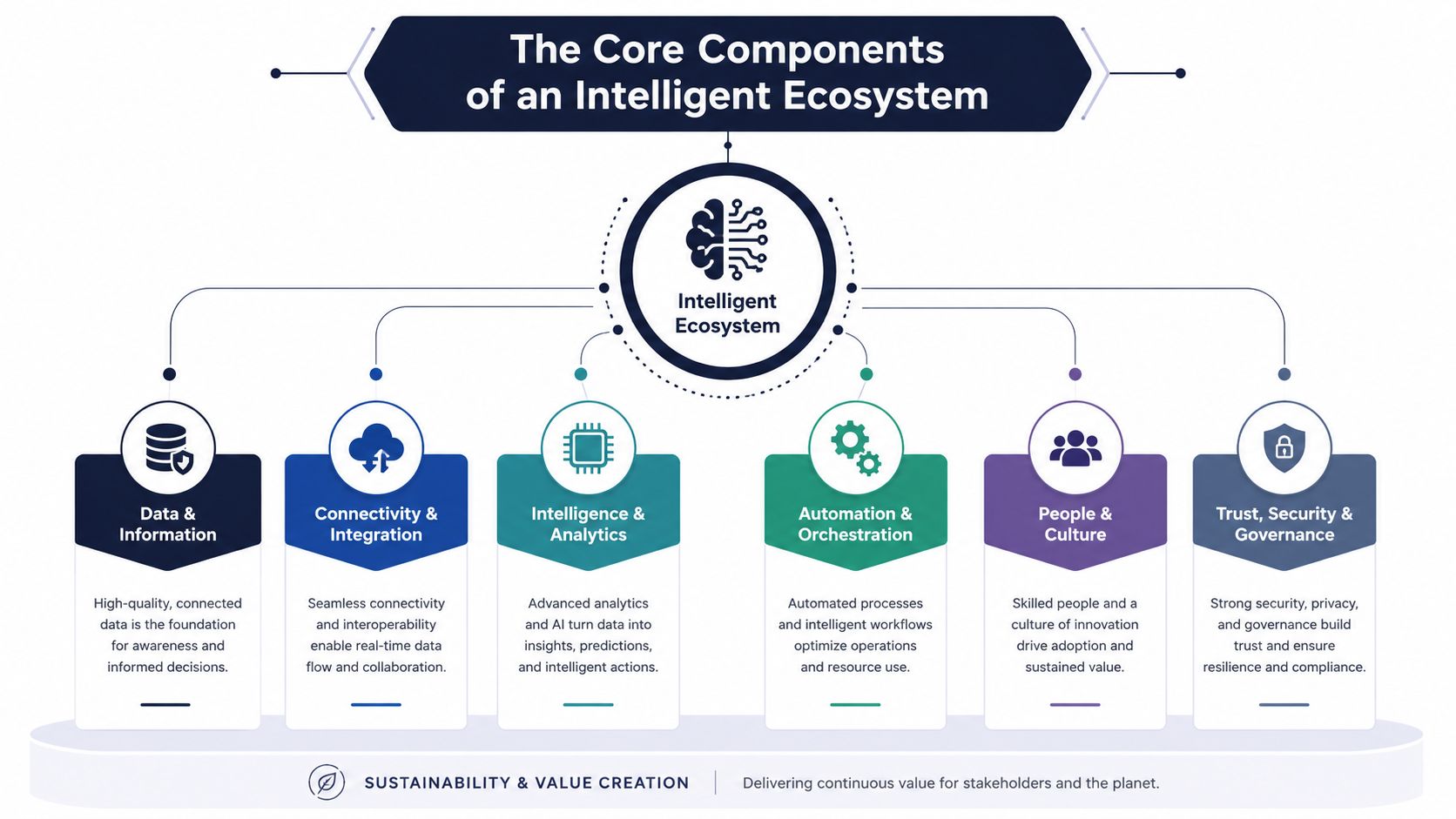
The five layers in plain language
Think of the ecosystem like a living body.
| Layer | What it does | Simple analogy |
|---|---|---|
| Data Connectivity | Moves data between EHRs, labs, wearables, telehealth tools, and other systems | Circulatory system |
| Intelligence | Uses AI and analytics to detect patterns, risks, and opportunities | Brain |
| Automation | Triggers actions such as alerts, scheduling, routing, or supply decisions | Nervous system |
| Experience | Gives patients and clinicians interfaces they can actually use | Face and hands |
| Governance and Ethics | Enforces privacy, bias controls, accountability, and compliance | Immune system |
The order matters. Teams often want to jump to the brain. They want prediction, copilots, or personalized recommendations. But if the circulatory system is weak, the brain gets poor signals.
That's where, as we explored in our guide to healthcare data fabric and unifying siloed data, the first hard truth shows up. Interoperability isn't plumbing in the background. It determines whether every later layer is useful or noisy.
Where leaders usually get confused
The most common confusion is treating these layers as separate products instead of interdependent capabilities.
-
Data connectivity isn't just integration work: It defines whether one patient has one coherent story or fragmented records across systems.
-
Intelligence isn't just model accuracy: It's whether the model answers a useful operational or clinical question at the right moment.
-
Automation isn't just workflow tooling: It decides whether insights create action or die in a dashboard.
-
Experience isn't just UI polish: It determines whether clinicians trust recommendations and whether patients stay engaged.
-
Governance isn't legal cleanup after launch: It shapes what data you can use, how models are monitored, and whether decisions are explainable.
A chronic care product is a good example. If a patient logs symptoms, uses a connected device, receives guidance, and triggers alerts before deterioration, every layer is involved. For teams thinking about patient engagement patterns, empowering patients with chronic care software is a useful companion read because it grounds the user side of what can otherwise sound like architecture jargon.
Good ecosystem design doesn't ask, “What can our AI do?” It asks, “What coordinated action becomes possible when data, workflow, and trust are aligned?”
That's the mindset behind successful custom healthcare software development. You aren't assembling modules. You're building a system that senses, decides, and acts.
Architecting for Intelligence, Security, and Compliance
Most failed health AI programs don't fail because the idea was bad. They fail because the architecture couldn't support actual constraints of healthcare. Privacy rules, legacy systems, audit needs, latency requirements, and workflow dependencies show up fast.
That's why the architecture for intelligent healthcare ecosystems has to be designed as a hybrid from the beginning. According to the VER journal paper on intelligent healthcare ecosystem architecture, effective ecosystems follow SMART principles: Stakeholder-oriented, Multi-layered, Adaptive, Real-time, and Trustworthy. The same source explains that these ecosystems use adaptive data integration and autonomous learning systems such as federated learning and edge AI to preserve privacy while supporting continuous model improvement.

What hybrid architecture means in practice
A hybrid architecture accepts that not all health data should move to one place, and not all intelligence should run in one environment.
Some decisions work well in centralized systems. Population analytics, historical trend analysis, and model training often need broad datasets. Other decisions belong closer to the edge. A bedside device, a remote monitoring endpoint, or a clinical workstation may need to process signals quickly and privately without waiting on a round trip to a central cloud environment.
That's why mature teams combine several patterns:
-
Standardized APIs and FHIR-based exchange so systems can communicate without brittle custom mappings
-
Federated learning when organizations need models to learn across distributed data without pooling sensitive records into one repository
-
Edge AI where low-latency or privacy-sensitive interpretation matters
-
Event-driven workflows so insights trigger action instead of becoming static reports
For readers mapping technical decisions to delivery work, this guide to healthcare data pipeline architecture is a practical reference point.
Why compliance must be built in
In healthcare, “secure by design” can't be a slogan. It has to shape schema design, access controls, consent handling, audit trails, and model governance. HIPAA and GDPR compliance don't sit on top of the stack. They influence the stack.
Here's a simple way to test whether the architecture is mature enough:
-
Can the team explain where each data element came from?
-
Can they restrict access by role, purpose, and context?
-
Can they show how a model was trained, updated, and monitored?
-
Can they isolate failures without shutting down the entire workflow?
If the answer is no, the platform may still work in a demo environment, but it won't scale safely.
The best healthcare architecture is boring in one important way. It makes the risky parts predictable.
Success or failure for many custom software development efforts often hinges on gaining traction or accumulating hidden risk. Healthcare organizations don't need systems that are only smart. They need systems that are dependable under pressure and ready for real healthcare integrations.
The Critical Role of Data Governance and Ethics
Most conversation about intelligent healthcare ecosystems starts too late in the chain. It starts with AI features, predictive care, virtual assistants, or digital twins. The harder truth is simpler. If the data is incomplete, biased, poorly labeled, or governed inconsistently, the intelligence layer will amplify those flaws.
That's not a theoretical concern. The Atlantic Council analysis on AI ecosystems in low- and middle-income economies argues that many narratives oversell healthcare AI's promise while ignoring a critical prerequisite, especially in LMICs: the lack of representative datasets. Without robust, population-representative data repositories, AI-enabled solutions can suffer from algorithmic bias and fail to achieve economic feasibility or improve national outcomes.
Why governance comes first
Leaders often hear “garbage in, garbage out” and treat it like a cliché. In healthcare, it's a patient safety issue.
A model trained mostly on one population may perform poorly on another. A risk score built from inconsistent coding may misprioritize patients. A recommendation engine may look accurate in development and become unreliable in production because source systems changed their documentation habits.
Good governance means deciding, before scale:
-
What data is authoritative for each clinical or operational domain
-
How records are normalized across facilities, vendors, and devices
-
Who owns data quality when fields are missing, delayed, or contradictory
-
How bias is assessed before and after deployment
-
What fallback behavior exists when the model confidence is weak
The overlooked challenge in global and multi-network products
This issue becomes sharper when companies build products meant to travel across regions, provider networks, or payer environments. Teams often assume a model that works in one setting can be transferred with minor tuning. It usually can't.
Different populations produce different baseline patterns. Different workflows create different documentation behavior. Different infrastructure leads to different data completeness. That's why governance isn't only about security and permissions. It's about representativeness and context.
A useful benchmark for how organizations communicate privacy responsibilities to users can be seen in How Rx360 safeguards your information. The lesson isn't to copy a policy template. It's to recognize that trust is built when data handling is explicit, understandable, and operationalized.
Watch for this trap: teams often try to fix bias at the model layer when the deeper problem sits in collection, labeling, or coverage gaps.
What ethical implementation looks like
Ethical AI in healthcare is less about lofty statements and more about operating discipline.
-
Collect broadly enough to reflect the populations you intend to serve
-
Document assumptions behind labels, exclusions, and thresholds
-
Review outputs with clinicians who understand edge cases
-
Monitor drift continuously because real-world populations and workflows change
-
Create appeal paths when users need to challenge or override model-driven recommendations
That's the unglamorous work. It's also the work that determines whether intelligence is safe, equitable, and worth deploying.
A Phased Roadmap for Ecosystem Implementation
Organizations usually get into trouble when they treat ecosystem building like a single transformation program with one launch date. Intelligent healthcare ecosystems mature in stages. The more practical way to approach them is through the three-phase model described in KPMG's framework for AI value creation in healthcare: Enable, Embed, and Evolve.
Enable
This is the foundation phase. It tends to be less visible and more important than executives expect.
The work here includes defining governance, mapping source systems, establishing interoperability priorities, clarifying consent and compliance requirements, and building the internal skills to own AI-enabled workflows. Teams also decide which data should be centralized, which should stay local, and how quality issues will be detected.
Without this phase, later pilots become expensive prototypes.
Embed
The second phase is where intelligence moves into daily operations. Instead of standing up isolated AI experiments, teams integrate capabilities into real workflows such as triage, imaging review, chronic care follow-up, scheduling, claims handling, or care navigation.
This stage usually forces uncomfortable product decisions. Which recommendations deserve interruptive alerts? Which should stay passive? When does automation help clinicians, and when does it create noise?
A practical implementation checklist often includes:
-
Workflow fit: Place recommendations where clinicians or staff already work
-
Change management: Train users on what the system does and does not do
-
Monitoring: Track whether the workflow improves action, not just model output
-
Fallback paths: Preserve safe manual operation when data feeds fail or confidence drops
This is also where an AI implementation roadmap becomes useful. Not as a presentation artifact, but as a decision framework tied to delivery milestones.
Evolve
In the third phase, the organization starts operating like an ecosystem rather than a collection of tools. Clinical, operational, and financial workflows begin to learn from each other. Insights from one part of the network inform decisions in another. Governance matures from project oversight into an operating discipline.
The shift is cultural as much as technical. Teams move from “Where can we add AI?” to “How should this organization learn and adapt across the full care journey?”
That maturity also affects delivery choices. Early phases may favor constrained pilots with specialist teams. Later phases often need broader software development service models, stronger platform ownership, and tighter product management across clinical, data, and operations functions.
For startups and scale-ups building platforms in this space, the lesson is straightforward. Don't promise an ecosystem in version one. Build the foundation, embed in the workflow, then earn the right to evolve.
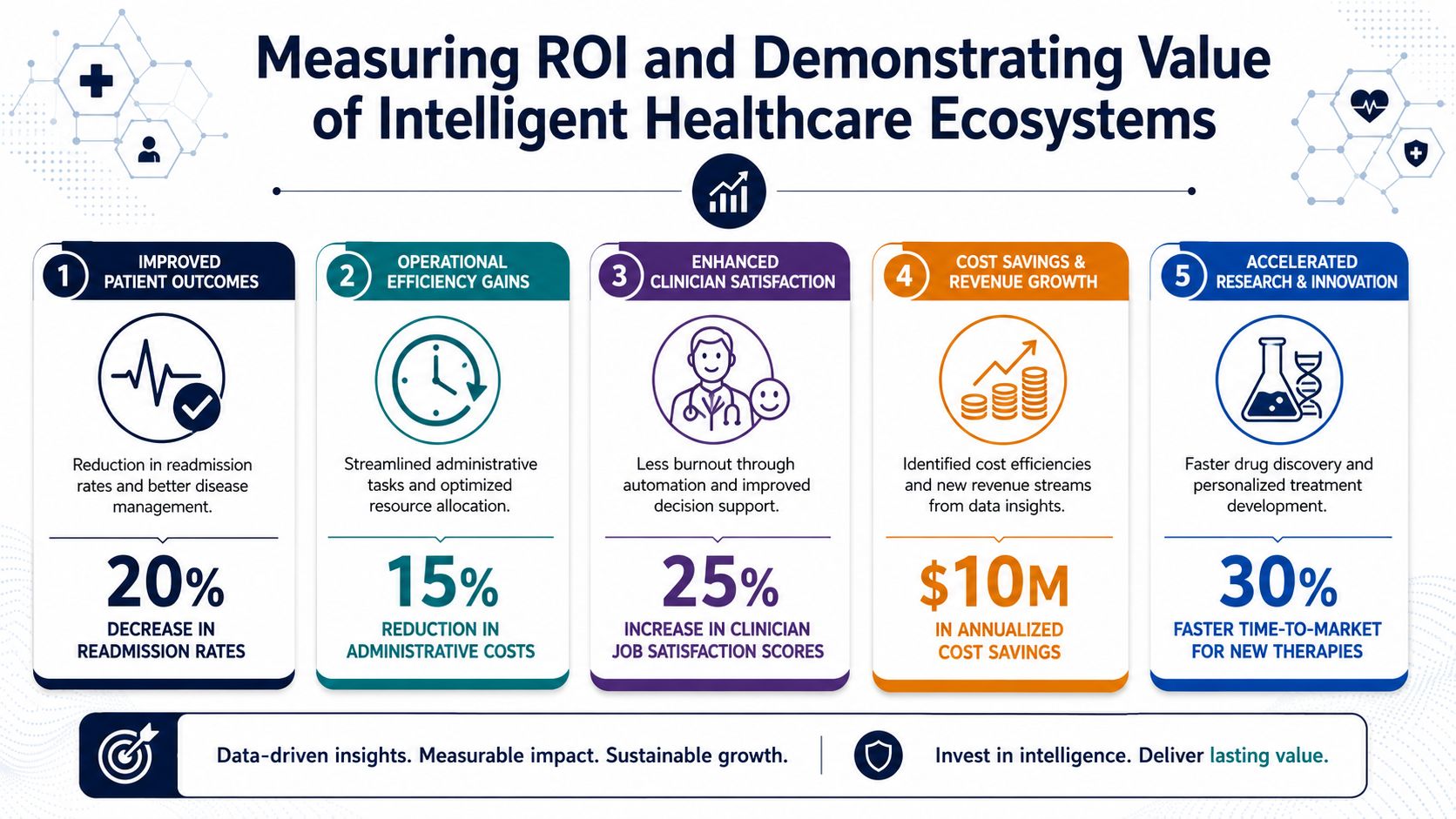
Measuring ROI and Demonstrating Value
Healthcare leaders rarely struggle to imagine possible value. They struggle to prove enough value, in operational and financial terms, to justify the complexity. ROI for intelligent healthcare ecosystems only becomes credible when the measurement model spans care quality, access, and cost at the same time.
That's the significance of the simulation described in the arXiv paper on an Intelligent Healthcare Ecosystem. It projects that an Intelligent Healthcare Ecosystem can reduce per-capita healthcare spending by 10 to 15 percent while simultaneously expanding access to care, driven by digital efficiencies, waste reduction, and a drop in preventable hospital readmissions for chronic conditions.
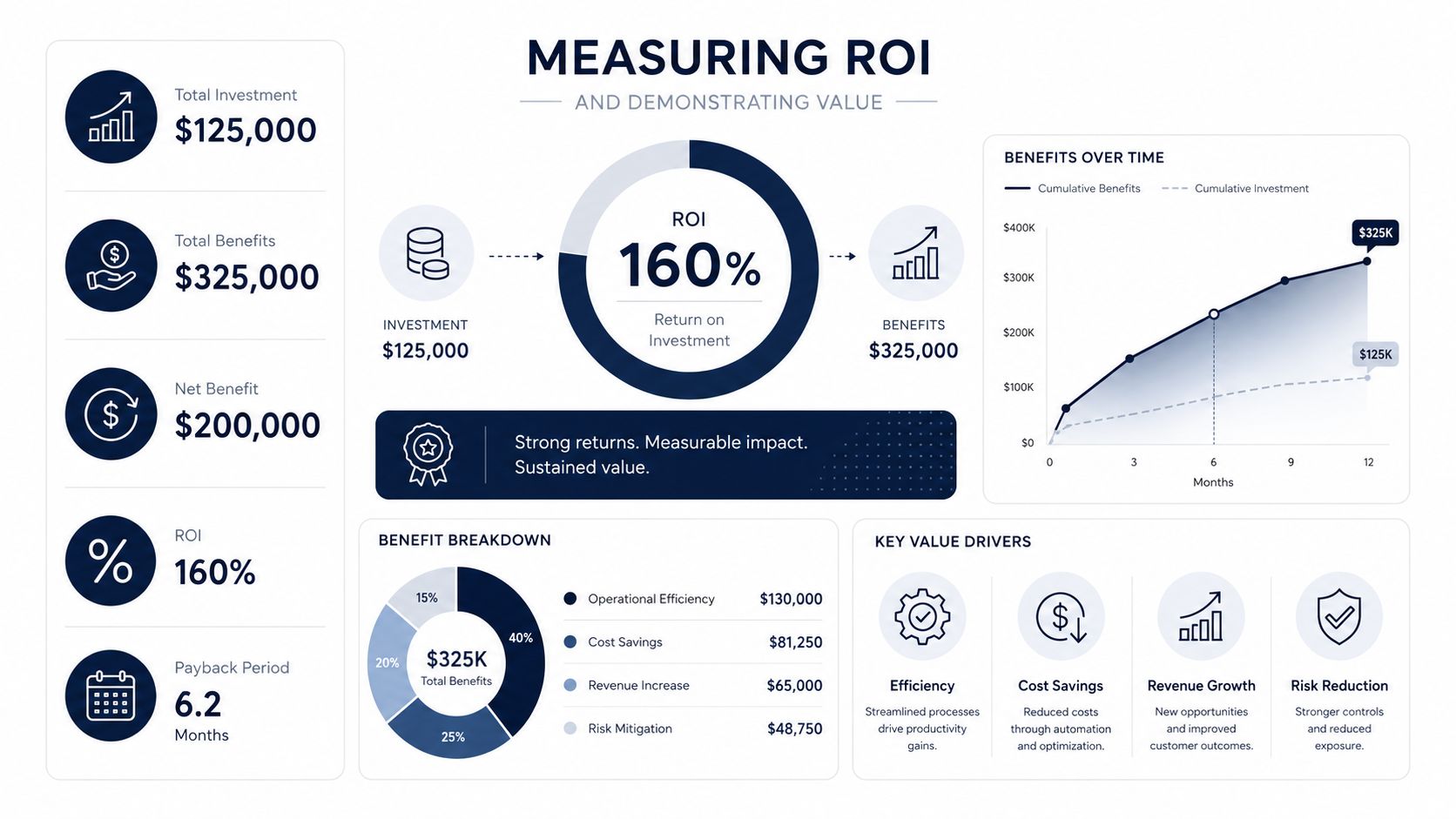
What ROI should include
The mistake many teams make is focusing on one headline metric. They measure one pilot outcome and call it a business case. Ecosystem ROI is broader.
A stronger scorecard usually tracks value across three domains:
| Domain | What to measure qualitatively | Why it matters |
|---|---|---|
| Clinical | preventable readmissions, earlier interventions, adherence, triage quality | Shows whether intelligence changes care, not just reporting |
| Operational | scheduling efficiency, staff coordination, admin burden, throughput reliability | Reveals whether workflow friction is going down |
| Financial | avoidable waste, claims friction, cost containment, service reach | Connects platform investment to budget outcomes |
The value often appears first in operations. Teams notice fewer manual handoffs, cleaner coordination, and less rework. Clinical and financial gains follow when those workflow improvements are sustained.
How to make the case internally
Executives and boards usually respond better to linked mechanisms than to abstract promises. Don’t say “AI will transform care.” Say this instead:
-
Connected data creates earlier visibility into risk
-
Workflow automation reduces avoidable delay and manual effort
-
Patient-facing digital channels extend access beyond physical settings
-
Coordinated interventions lower acute escalation and wasted spend
That’s a more believable chain of value.
For leaders working on advanced platform investments, as we explored in our guide to healthcare digital twins, AI, and ROI the strongest business cases show how a capability changes the operating model, not just a report or dashboard.
ROI in healthcare is strongest when one capability does three jobs at once. It improves a patient journey, removes staff friction, and lowers avoidable cost.
This is where enterprise AI solutions and focused AI development services need discipline. The goal isn’t to deploy more AI. It’s to invest in capabilities that compound across the ecosystem.
Intelligent Healthcare in Action Use Cases
The fastest way to understand intelligent healthcare ecosystems is to follow the people using them.
A patient managing chronic disease at home
A patient with a long-term condition uses a mobile app, a connected monitoring device, and a care team portal. Their readings don’t just sit in a graph. The platform interprets trends, compares them with prior patterns, and prompts outreach when the trajectory looks concerning.
The patient doesn’t need to understand the architecture. They feel the outcome. Fewer unnecessary visits, more timely check-ins, and guidance that feels connected rather than generic. This is also why many healthtech startups pair remote monitoring with SaaS product development, because subscription platforms are often the delivery model for longitudinal care experiences.
A radiologist working with AI support
A radiologist reviews imaging in a workflow where machine learning helps flag abnormalities and prioritize review order. The system doesn’t replace judgment. It reduces scanning fatigue and helps surface cases that deserve attention sooner.
The key design choice here isn’t only model performance. It’s workflow placement. If the output appears in a separate application, the clinician may ignore it. If it appears in the existing review context with clear rationale and appropriate confidence cues, it becomes useful.
An operations leader managing hospital flow
A hospital administrator opens a dashboard that combines bed status, staffing constraints, expected demand, discharge readiness, and scheduling pressure. The system suggests reallocations and highlights bottlenecks before they become visible in daily chaos.
That’s where the ecosystem starts to feel different from a reporting stack. It doesn’t just describe what happened. It helps teams coordinate what should happen next.
For leaders evaluating what mature delivery can look like in adjacent transformation programs, reviewing real client cases can help ground product strategy in operational reality.
The pattern across all three examples is consistent. Intelligence matters. But ultimate value comes from connecting data, decisions, and action around a person or workflow.
Frequently Asked Questions
Is an intelligent healthcare ecosystem the same as a hospital platform?
No. A hospital platform can be one part of the ecosystem, but the ecosystem extends across settings, stakeholders, and workflows. It includes care delivery, operations, patient engagement, and often payer or claims-related processes.
Where should a CTO start?
Start with data governance and interoperability, not the flashiest AI use case. If your data sources don’t align, the intelligence layer will be fragile and hard to trust.
Does every organization need advanced AI on day one?
No. Many teams should begin with connected data, workflow visibility, and targeted automation. AI becomes more valuable when the underlying system is stable enough to support it.
What’s the biggest implementation mistake?
Treating the initiative as a model deployment instead of an operating model change. Most failures come from weak workflow integration, poor data quality, or lack of clear accountability.
How do you prevent algorithmic bias?
You can’t solve it with one technical fix. You need representative datasets, careful labeling, governance rules, clinical oversight, and ongoing monitoring after deployment.
How should product leaders think about architecture decisions?
Choose architecture based on workflow, privacy, and reliability needs. Some intelligence belongs in centralized environments. Some belongs closer to the edge. The right answer is usually hybrid.
Can startups build in this space without huge infrastructure budgets?
Yes, but they should narrow the first scope. Pick one workflow, prove trusted data movement, embed into real user behavior, and avoid pretending that a single app is already an ecosystem.
Bridge Global helps organizations build compliant, scalable healthtech platforms with AI, interoperability, and product engineering discipline. If you’re planning intelligent healthcare ecosystems, need a stronger custom software development strategy, or want an experienced healthtech software development partner for healthcare-grade delivery, Bridge Global is a practical place to start.
About Upendra Jith
Upendrajith completed his Master's in English and has been a commercial content developer for the past three years. He's more inclined to develop content with a 'street-smart' delivery on topics such as technology, media, or anything he can get his hands on. He has a fixation on lyrics, dark poetry, media, technology, and flow arts.
View all posts by Upendra Jith →