

Healthcare Data Fabric: How to Unify Siloed Data
Healthcare organizations don't have a data shortage. They have a data access problem. According to an IDC study, healthcare data is projected to grow at a 36% compound annual growth rate through 2025, faster than any other industry, and hospitals now produce over 50 petabytes of data annually, yet 95% remains unused or unanalyzed. That gap is why the idea of a healthcare data fabric matters.
For CTOs building platforms for providers, payers, or digital health products, the question isn't whether more systems will appear. They will. The question is whether your architecture can connect EHR data, claims files, imaging, device streams, and operational records without creating another brittle integration mess. A healthcare data fabric gives you a way to weave those threads together while keeping governance, security, and performance intact.
The Data Deluge in Healthcare and Why It Demands a New Approach
Healthcare creates more data than many architectures were ever designed to handle. The problem is not only volume. It is fragmentation across EHRs, radiology systems, claims platforms, pharmacy feeds, lab tools, device streams, and scanned documents, each with its own format, latency, and access rules.
For a CTO, that fragmentation shows up in very practical ways. A clinician asks for a current medication view. A care manager needs the recent admissions and claims context. A finance team wants to reconcile charges against documentation. The answer may exist, but it is scattered across systems that were purchased at different times, for different departments, with different assumptions about identity, data standards, and retention.
Woven fabric is a useful comparison here. Individual threads matter, but they only become durable when they are connected with structure and tension in the right places. Healthcare data works the same way. A lab result, an eligibility file, or a discharge summary has limited value in isolation. Clinical and business value appear when those pieces can be found, interpreted, trusted, and governed together.
Poorly connected data quickly becomes an operational risk. It contributes to billing delays, reporting gaps, duplicated work, care coordination errors, and audit exposure.
Data quality also becomes a patient-safety issue, not just an analytics issue. If you want a grounded view of what fragmented and inconsistent records can lead to, the examples of poor data quality in healthcare are worth reviewing.
Many organizations respond by adding another interface, another ETL job, or another repository. That approach usually increases complexity. Each new connection solves one local problem while creating another dependency to monitor, secure, map, and maintain. Over time, integration turns into a patchwork that is expensive to change and hard to validate for HIPAA, audit trails, consent handling, and data lineage.
That last point is often missed in vendor marketing. In healthcare, an architecture is not production-ready because it can connect systems in a demo. It has to prove that data provenance is traceable, access controls are enforceable, policy rules are consistent across sources, and quality checks can stand up to compliance review. It also has to show measurable outcomes, such as fewer reconciliation hours, faster prior authorization workflows, better care coordination, or cleaner reporting for value-based care.
A better approach starts with the access model:
Point-to-point integrations add fragility: Every new feed creates another mapping, failure point, and maintenance burden.
Centralizing copies of everything creates governance problems: Duplicated data often drifts from the source and complicates retention, access control, and auditability.
A logical data layer supports scale: It connects distributed sources, applies shared rules, and gives teams a consistent way to use data without constant re-platforming.
That is the architectural pressure pushing healthcare organizations toward a different model. They need a way to connect distributed data, test it against real compliance requirements, and measure whether the architecture improves both clinical workflows and financial performance.
What Is a Healthcare Data Fabric
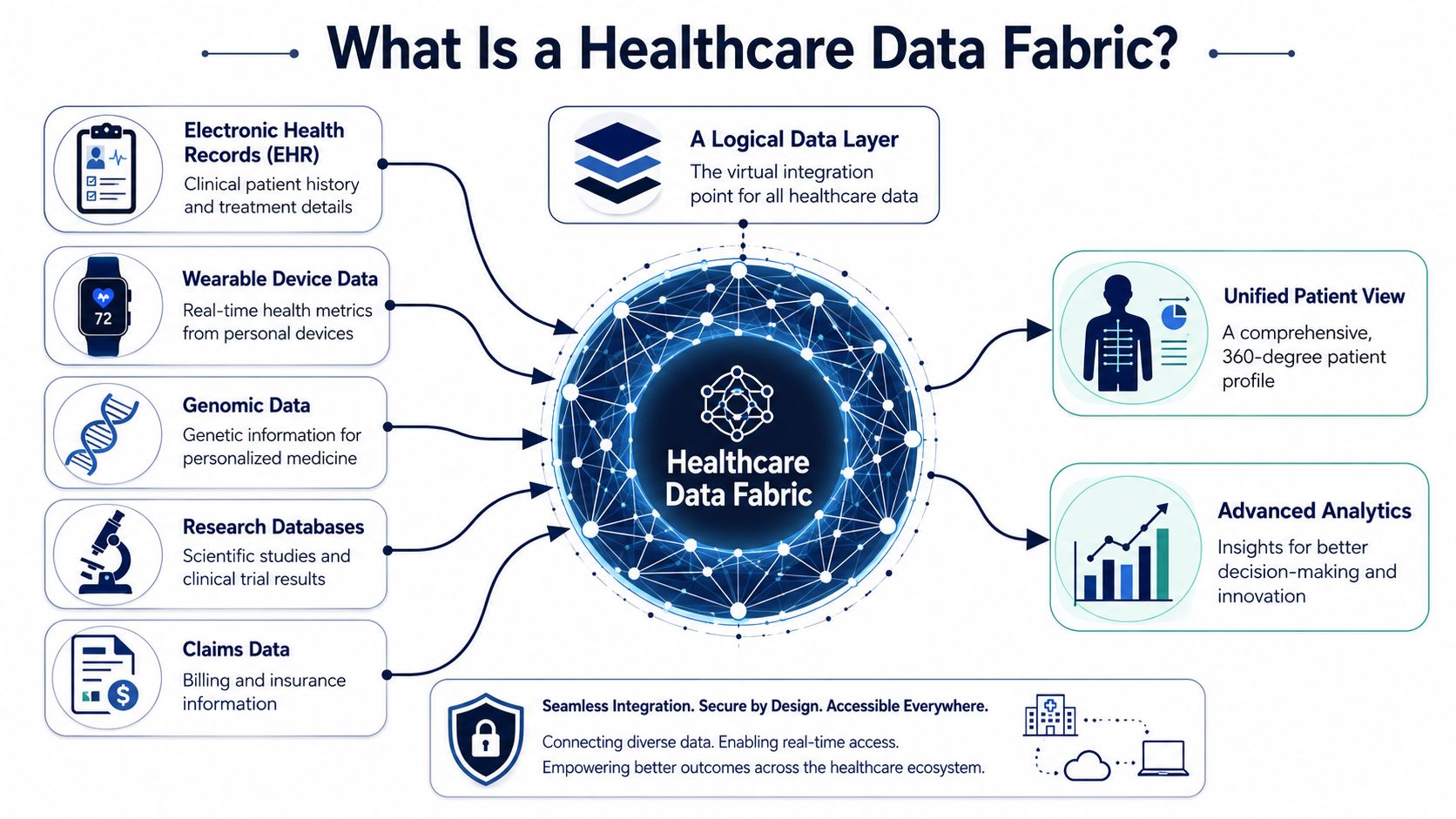
A healthcare data fabric is an architectural model for connecting distributed healthcare data without forcing every source into a single repository first. It creates a governed access layer across EHRs, claims platforms, imaging systems, lab feeds, CRM tools, and partner data so applications and analysts can work from consistent rules, definitions, and policies.
The easiest way to understand it is through the fabric analogy itself. Threads stay separate, but the weave gives them structure. In the same way, source systems keep their own operational role, while the fabric binds them through metadata, semantics, orchestration, and access controls.
That matters in healthcare because the problem is not just volume. It is a variation. An HL7 ADT feed, a FHIR API response, a scanned referral, a prior authorization record, and imaging metadata all describe patient activity differently. Without a unifying layer, every new workflow becomes another custom build, another mapping exercise, and another compliance review. Teams building data and AI solutions for healthcare operations run into this when they need a usable patient, provider, or member view across disconnected systems.
A data fabric also changes how leaders should evaluate architecture. The key consideration is not whether a platform can connect systems in a product demo. Rather, it is whether it can prove lineage, enforce policy consistently, support consent and retention rules, and produce evidence that the architecture improves outcomes in production. That validation gap is where many healthcare programs stall.
The market reflects that shift. Analysts at Fortune Business Insights reported that the global data fabric market was valued at an estimated USD 3.37 billion in 2025 and is projected to reach USD 16.46 billion by 2034, with a 21.90% CAGR (Fortune Business Insights).
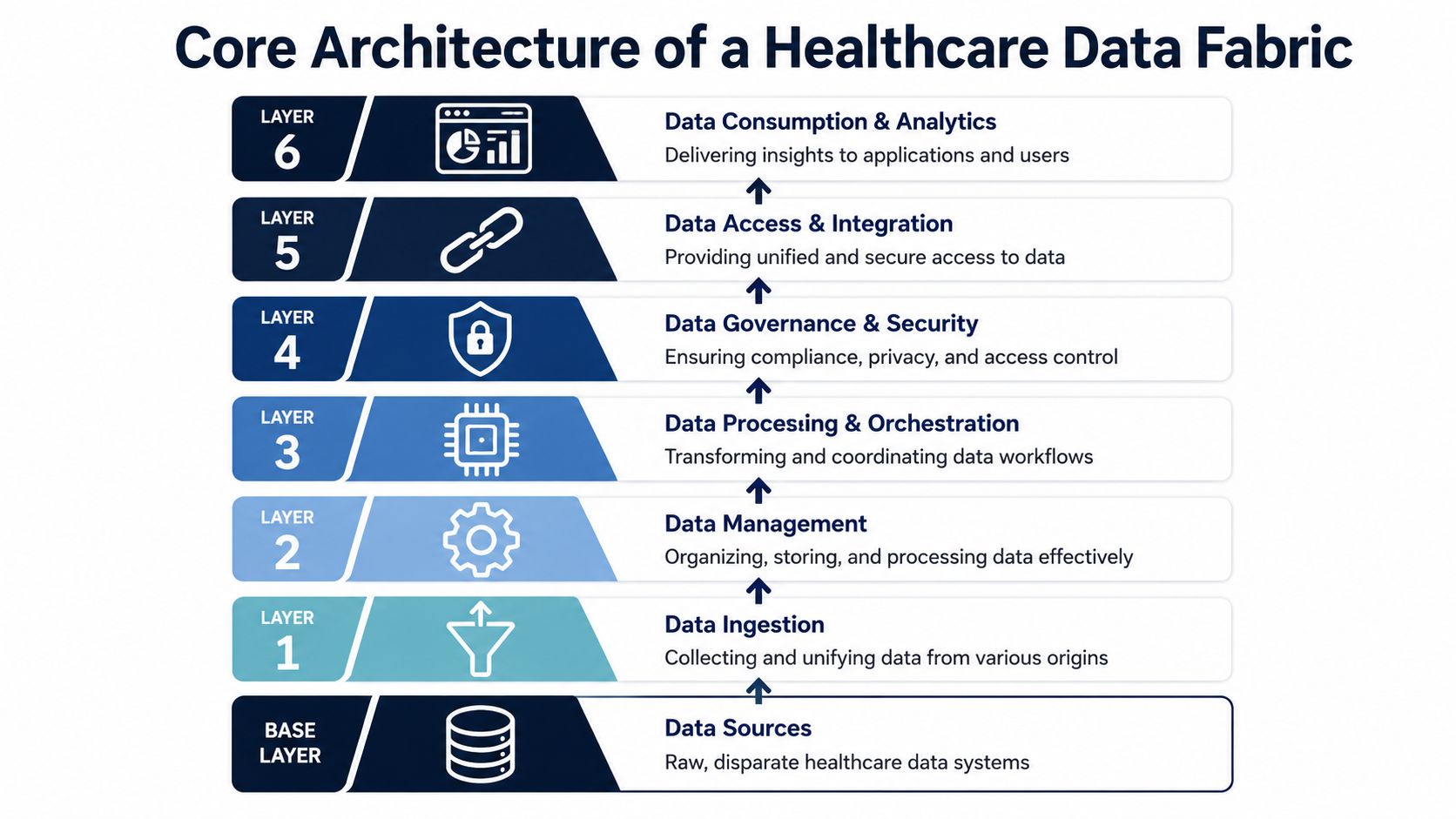
The six layers in plain English
A useful way to examine a fabric is layer by layer, because each layer answers a different operational question.
Data Management: Defines stewardship, security, lineage, retention, and policy enforcement.
Data Ingestion: Connects feeds, files, event streams, and APIs from internal and external systems.
Data Processing: Cleans, transforms, matches, and prepares raw data for downstream use.
Data Orchestration: Coordinates workflows, rules, triggers, and handoffs across systems.
Data Discovery: Helps teams find available data assets, understand context, and assess reuse.
Data Access: Delivers trusted data to applications, analytics tools, and operational services.
Together, these layers support active metadata, semantic mapping, and shared policy enforcement. That is particularly important in healthcare, where terminology alignment is tied directly to interoperability, reporting quality, and auditability. If your team is working through coding systems, mappings, and normalization, this guide on mastering healthcare data standards adds useful context.
How it differs from a lake or warehouse
A data lake or warehouse still serves an important role. Many organizations need one for historical reporting, training models, and large-scale analytics. A healthcare data fabric addresses a different architectural need. It makes distributed data usable and governable across operational systems.
| Approach | Primary role | Common limitation in healthcare |
|---|---|---|
| Data warehouse | Centralized analytics store | New source onboarding and workflow changes can be slow |
| Data lake | Large-scale raw data storage | Governance, terminology control, and trust can drift over time |
| Healthcare data fabric | Governed access and coordination across systems | Success depends on strong metadata, policy design, and operational discipline |
A warehouse stores the cloth. A fabric weaves the threads so teams can use them with confidence. In healthcare, that difference affects more than architecture diagrams. It affects whether compliance teams can verify controls, whether care teams can trust the record in front of them, and whether finance leaders can tie the investment to fewer manual reconciliations, faster workflows, and cleaner reporting.
Core Architecture and Key Components
A healthcare data fabric succeeds or fails at the architecture level. The question is not whether a vendor can show connectors, dashboards, or policy screens in a demo. The question is whether those parts work together under real operational pressure, with PHI controls, audit evidence, source system changes, and clinical uptime requirements all in play.
The fabric analogy matters here. A bolt of cloth is useful because individual threads are held together in a repeatable pattern. A healthcare data fabric works the same way. EHR feeds, claims files, imaging metadata, lab results, identity records, and access policies remain distributed, but the architecture weaves them into a governed operating model.
The layers and what they actually do
A practical way to assess a fabric is to examine each layer like a CTO preparing for production, not procurement.
Data management
This layer sets the operating rules. It covers stewardship, retention, lineage, classification, access policy, and evidence collection for audits. It is also the layer where compliance validation has to become concrete. For example, you would configure and test a rule that a user with a "clinician" role cannot access billing data, then generate an audit log showing the denied request, the policy applied, and who reviewed the control. If a vendor cannot show how those checks are tested and documented in your environment, the architecture is still theoretical.Data discovery
Discovery gives teams a map before they start weaving threads together. It profiles source systems, records schema changes, identifies join points across EMRs, billing platforms, imaging archives, and external partners, and captures business meaning in metadata. In healthcare, this layer reduces a common source of failure. Teams often connect systems successfully but still disagree on what a field means, which coding version applies, or which source is authoritative.Data ingestion
Ingestion brings data into the fabric through HL7, FHIR, flat files, APIs, device streams, and batch exports. The hard part is not just connectivity. It is making each feed repeatable, observable, and recoverable when a message format changes or a source goes offline. A production-ready design tracks what arrived, what failed, what was retried, and what downstream systems were affected.Data processing
Processing turns messy inputs into usable information. That includes parsing, normalization, deduplication, terminology alignment, enrichment, and data quality checks. In healthcare, small defects create expensive downstream consequences. A missing encounter identifier can break reporting. An unmapped code can distort quality measures. This layer needs explicit tests, not assumptions.Data orchestration
Orchestration manages timing and dependency. It determines what happens after a new admission message arrives, when a payer eligibility file lands late, or when a source system adds a new field without notice. Good orchestration protects the business from brittle point-to-point logic. It also gives operations teams a place to see failures, rerun workflows safely, and prove that controls executed in the right order.Data access
Access is how governed data reaches dashboards, care management tools, APIs, analytics platforms, and AI workflows. This layer should expose information according to policy, role, purpose, and context. The goal is not broad access. The goal is correct access, fast enough for operations and controlled enough for compliance.
Practical rule: If your team cannot name the owner, control points, and test method for each layer, the architecture is not ready for scale.
What a production-ready architecture looks like
Many articles stop at naming the layers. CTOs usually need a different answer. How do you know the design will hold up in a regulated environment?
Start with validation, not features. Ask the platform team to demonstrate policy enforcement with real roles, masked fields, denial events, and audit trails. Ask how lineage is captured when data is transformed or virtualized rather than copied. Ask how schema drift is detected, who gets alerted, and what happens to dependent workflows. Ask how retention and deletion policies are applied across distributed sources, not just in a central repository.
Those questions separate slideware from operating architecture.
This is also where investment decisions become clearer. Teams exploring data and AI services for healthcare operations often find that AI use cases stall for a simple reason. The model is not the first bottleneck. Data policy enforcement, metadata quality, and orchestration reliability are. A fabric earns its place when it reduces that friction while giving compliance and audit teams evidence they can verify.
Why the layers matter together
A weak layer affects every layer above it. If discovery is incomplete, processing logic will be fragile. If management policies are vague, access controls become inconsistent. If orchestration is immature, even high-quality data arrives at the wrong time or without the right approvals.
That is why a healthcare data fabric should be evaluated as an operating system for data, not a collection of integration features. The true measure is whether the architecture can support clinical use, financial reporting, and regulatory scrutiny at the same time.
Transformative Benefits for Healthcare Providers and Payers
A data fabric pays off when clinicians, operators, and finance teams stop spending their day stitching together conflicting records. For healthcare organizations, the gain is practical. Fewer duplicate data copies, faster access to trusted information, and less manual reconciliation across systems that were never designed to work together.
One benefit stands out early. Virtualized access can reduce redundancy by up to 40% and cut data access times from hours to milliseconds. In healthcare, that matters because a care manager, revenue cycle analyst, and compliance officer may all need the same underlying data, but in different forms and on different timelines.
The fabric analogy helps here. Traditional integration often works like sewing a new patch onto the same garment every time a department has a request. Eventually, the garment is hard to maintain. A data fabric works more like a managed weave. The threads stay where they are, but the organization gains a consistent way to find, govern, and use them across many workflows.
What changes for providers
Provider organizations usually feel the impact first in care delivery, reporting, and application delivery.
Clinical workflows: Care teams can work from a more complete view across EHR, imaging, labs, and ancillary systems without waiting for custom extracts.
Operational reporting: Analysts spend less time validating spreadsheet versions and more time using governed datasets with known lineage.
Digital product delivery: Patient portals, clinician tools, and internal dashboards can draw from shared data services instead of one-off interfaces.
That third point often drives more value than teams expect. If each new app requires a fresh integration project, delivery slows, costs rise, and policy enforcement becomes inconsistent. A fabric changes that pattern by reusing the same governed data foundation across products.
What changes for payers
Payers see a different set of gains, but the pattern is similar. Eligibility files, claims feeds, provider rosters, prior authorization events, and member data often arrive in different formats and on different schedules. A data fabric does not remove that complexity. It gives teams a repeatable way to organize it, apply quality rules, and serve downstream systems without rebuilding the same mapping logic every quarter.
That has direct operational value. Claims operations can process cleaner inputs. Network teams can compare provider and contract data with fewer reconciliation loops. Finance teams can trace how a number moved from the source file to the report, which matters when an audit or payment dispute lands on the desk.
Strong ROI usually begins with a painful operational bottleneck. Better clinical and financial outcomes appear when organizations measure the effect on readmissions, denial rates, care gap closure, call center handling time, or days in A/R, rather than stopping at technical metrics.
A sensible rollout pattern
The strongest programs start where friction is visible and measurable.
Choose one narrow workflow: Admissions events, care gap reporting, claims file normalization, or provider directory synchronization are good starting points.
Prove shared, governed use: Show that one trusted dataset can support clinical, operational, and financial users without creating new copies for each team.
Measure outcomes, not only throughput: Track whether the fabric improved a real business result, such as faster discharge coordination, fewer claim exceptions, or less analyst time spent on reconciliation.
Validate production readiness early: Confirm that lineage, access controls, audit evidence, and policy enforcement hold up under regulated workloads, not just in a vendor demo.
That last step is often overlooked in articles about data fabric. Healthcare leaders need more than architecture diagrams and feature lists. They need proof that the model can stand up to compliance review and proof that it changes outcomes in practical settings. Those two tests separate an interesting platform from an operating capability.
Your Practical Implementation Roadmap
A healthcare data fabric rollout succeeds or fails on one question: can your team prove, with evidence, that the platform is safe and reliable enough for regulated production use?
That question should shape the roadmap from day one. A data fabric works like a woven fabric. The value does not come from a single thread, such as a connector, a lakehouse, or a catalog. It comes from how the threads are joined and how well the weave holds under strain. In healthcare, the strain is real. Audits, claims disputes, source-system changes, privacy reviews, and downtime events all test whether the architecture works outside a demo.
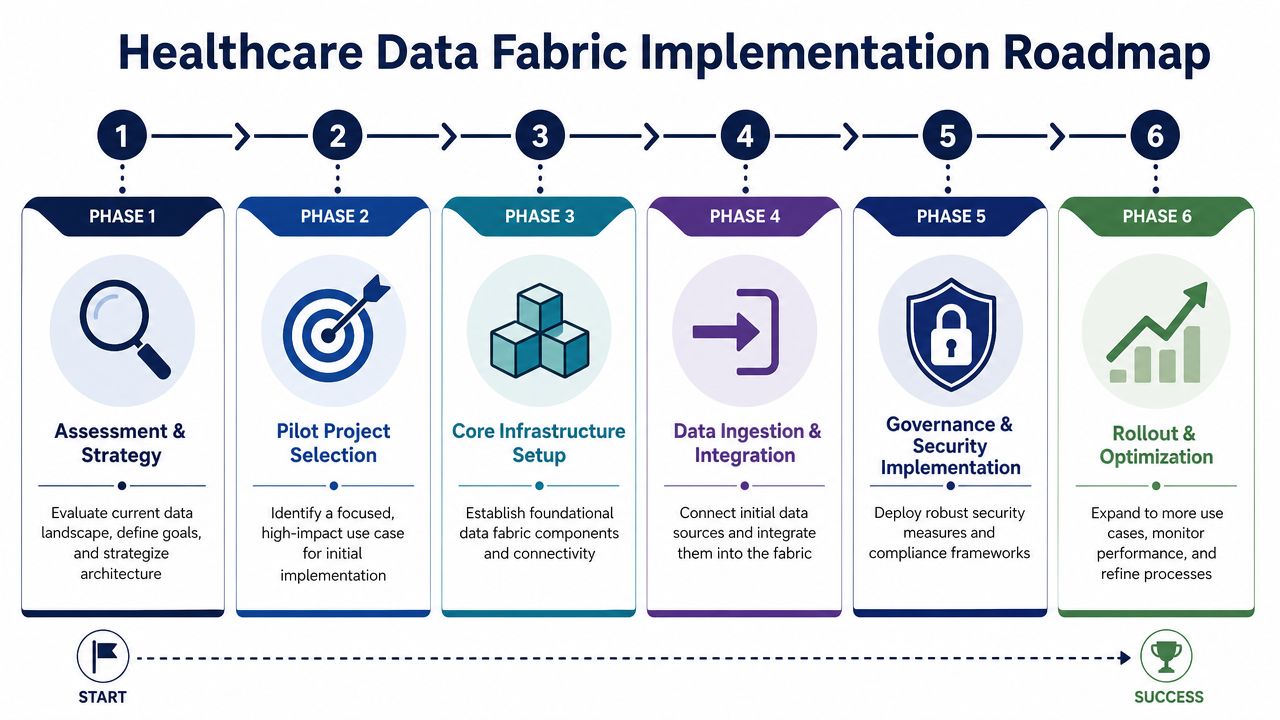
Phase 1 and Phase 2
The first two phases set the boundaries. That matters because healthcare teams often start too wide, then spend months connecting systems without proving business value or audit readiness.
Assessment and strategy: Inventory source systems, data contracts, current controls, business priorities, and decision points. Identify where clinical, financial, and operational data must meet. Separate workflows that need near-real-time data from those that work fine in batch.
Pilot selection: Choose one use case with visible cost, delay, or compliance friction. Good starting points include admission event visibility, payer file normalization, prior authorization status tracking, or a cross-system patient summary.
A pilot should answer three practical questions. Can the fabric deliver trusted data fast enough for the workflow? Can the organization control who sees what? Can the team produce evidence when compliance or operations asks for it?
Phase 3 and Phase 4
These phases create the pattern you will repeat.
Build the core platform
Start with the control layer. Set up metadata management, policy enforcement, orchestration, monitoring, and identity controls before scaling ingestion. If teams connect sources first and add controls later, the fabric becomes another patchwork of pipelines.
This is also the point to involve specialists in healthcare cybersecurity services, especially if the pilot touches PHI, payer data, or shared environments across business units.
Ingest and model carefully
Connect only the systems required for the pilot. Define shared business terms where confusion would break the use case, but avoid trying to normalize every code set and document type on day one. A good fabric strategy reduces integration debt in layers. It does not promise to settle every terminology dispute in the first release.
Production readiness depends less on feature count and more on evidence. Your team should be able to show how data moved, who accessed it, what changed, and how failures were handled under actual operating conditions.
Phase 5 and Phase 6
The later phases turn a successful pilot into an operating capability.
Governance and security implementation
Apply encryption, role-based access, audit logging, retention rules, environment separation, and change controls as part of the architecture. In healthcare, policy only matters if it produces usable proof.Rollout and optimization
Expand to adjacent domains after the pilot shows stable service levels, clear ownership, and measurable business results. Scale by repeating a tested pattern, not by adding sources faster than teams can govern them.
A practical readiness checklist should be concrete enough to test:
Lineage evidence: Can you produce a report showing every system, user, and pipeline that accessed Patient ID 12345 in the last 24 hours?
Access reviews: Can you show that a scheduler, claims analyst, and care manager each see only the fields required for their role?
Operational logs: After a failed pipeline at 2:13 a.m., can your team reconstruct what happened without searching across five tools?
Schema change handling: If a source adds or renames a field, does the fabric alert the team and contain the issue instead of passing bad data downstream?
Disaster procedures: Can you demonstrate recovery steps, recovery time, and data reconciliation with records from an actual test?
Change approval evidence: Can you show who approved a policy, mapping, or access-rule change and when it went live?
Data quality thresholds: Can you document the minimum completeness, timeliness, and match-rate standards required before data is used in care operations or payment workflows?
That level of specificity is where many articles stop short. Healthcare CTOs do not need another abstract maturity model. They need a roadmap that shows how to verify regulatory readiness in production and how to connect that readiness to outcomes such as fewer reconciliation hours, faster decisions, cleaner claims, or better care coordination. That is the difference between installing technology and building a fabric that the organization can trust.
Ensuring Security Compliance and Data Governance
In healthcare, architecture isn't credible unless compliance is built into daily operations. A healthcare data fabric helps because it creates one place to enforce policy across many systems, even when the underlying sources stay distributed.
The strongest implementations apply encryption for data at rest and in transit, granular role-based access controls, and automated lineage tracking so teams can support HIPAA-aligned operations and broader regulatory expectations around traceability and access discipline. That combination matters for claims files, clinical PDFs, enrollment rosters, and event-driven feeds, where the risk isn't only exposure. It's also uncontrolled reuse and weak audit trails.

Benchmark data from Microsoft Fabric implementations shows a 60% reduction in infrastructure duplication costs and a 70% reduction in manual processing time when systems are consolidated into a single fabric platform that enforces HIPAA compliance (Invene). Those figures are vendor-specific, but they illustrate an important principle. Security architecture can improve efficiency when it replaces overlapping tools and handoffs.
What governance looks like in practice
Governance in a healthcare data fabric usually rests on a few essential elements:
Identity-aware access: Users and services should get access based on role, purpose, and scope.
Lineage by default: Every movement, transformation, and exposure path should be traceable.
Policy centralization: Retention, masking, and access rules shouldn't be redefined in every downstream tool.
Structured ingestion controls: Incoming HL7 messages, CMS flat files, and similar formats need validation before analytics teams consume them.
Security leaders often partner closely with platform engineering. A mature fabric isn't just interoperable. It's inspectable. Teams evaluating broader security posture often need the same disciplines covered by dedicated cybersecurity services.
The compliance trap to avoid
Many teams assume a compliant cloud environment makes their data fabric compliant. It doesn't. Infrastructure certifications help, but auditors still want evidence about your configurations, your access model, your operational logs, and your incident handling process.
Compliance depends on what your team enforces and can prove, not only on what a vendor advertises.
Real-World Use Cases and Measuring True ROI
A healthcare data fabric earns budget approval when it changes daily operations in ways leaders can verify. Architecture diagrams rarely do that. Teams fund what they can see. Faster data access for care managers. Fewer manual reconciliations for payer operations. Cleaner inputs for reporting, analytics, and product teams.
The fabric analogy matters here. A single thread is useful, but limited. Woven together with rules about how threads connect, it becomes strong enough to carry weight. In healthcare, those threads are EHR events, claims, eligibility files, lab results, notes, and operational data. A data fabric ties them together with shared metadata, policies, and access patterns so one use case does not have to be rebuilt from scratch for the next.
Use cases that fit the model well
The best early use cases share one trait. They depend on data from multiple systems, but they also have a clear operational owner who can confirm whether the new approach works.
Care coordination workflows: ADT events can trigger follow-up tasks, outreach, or case review when the event arrives in a usable format and reaches the right workflow on time.
Payer data operations: Claims, enrollment, authorization, and roster data become easier to query and reconcile when teams apply one set of ingestion and metadata rules instead of patching each feed separately.
Population health analysis: Analysts can study clinical and administrative patterns together without waiting for separate domain-specific extracts.
AI-enabled applications: Summarization, risk detection, and clinical support tools depend on governed access to both structured records and unstructured content. AI development services become practical only when the underlying data is traceable, permissioned, and ready for production use.
Healthcare product companies see the same pattern. Multi-tenant platforms need repeatable integrations, tenant-aware governance, and a shared data layer that can handle variation without turning every customer request into custom engineering.
The evidence gap leaders should address directly
Many articles conclude prematurely. They jump from architecture to outcomes and imply a straight line from data fabric adoption to lower readmissions or better value-based care performance. For most organizations, that line is not direct, and proving it takes time.
A production-grade evaluation should answer two separate questions.
First, can the fabric stand up to real compliance scrutiny, not just a vendor demo? That means testing lineage, access enforcement, audit evidence, retention behavior, and incident response in live operating conditions.
Second, does the fabric improve clinical and financial performance through measurable operational change? If data still arrives late, if workflows still rely on manual rework, or if users do not trust what they see, the architecture has not delivered business value yet.
A practical way to measure ROI
Start with one use case, one accountable owner, and one baseline. Then measure the chain of impact in order, like tracing a thread through cloth. If the first stitch fails, the finished fabric will not hold.
| ROI layer | What to measure qualitatively | Why it matters |
|---|---|---|
| Operational | Time to onboard sources, effort to prepare data, speed of access, manual handoffs | Shows whether the fabric is removing friction from day-to-day work |
| Governance | Audit traceability, access review clarity, policy consistency | Shows whether compliance work is becoming easier to prove and maintain |
| Product delivery | Speed of feature delivery, reuse of shared data services | Shows whether engineering is becoming more efficient |
| Outcome tracking | Changes in intervention timing, reporting quality, and downstream care or financial metrics | Shows whether operational improvement is affecting business performance |
That order matters. Clinical and financial outcomes sit at the far end of the chain. They should be measured, but they should not be the first proof point. The first proof point is whether the right data reaches the right person or system in time to change an action.
How to make ROI credible to clinical, financial, and compliance stakeholders
A credible ROI model separates architecture impact from program impact.
If a care management team can identify discharge events sooner, assign follow-up faster, and document outreach more consistently, that is architectural value with observable evidence. Whether those changes later affect readmissions depends on staffing, workflow design, patient engagement, and clinical execution as well.
A few rules help keep the measurement honest:
Validate production controls early: Run access reviews, lineage checks, and audit-log tests before calling the platform compliant.
Prove workflow improvement before outcome improvement: Confirm that the fabric changes speed, completeness, or trust in the workflow itself.
Measure adoption behavior: If analysts export data to spreadsheets or clinicians avoid the outputs, the technical implementation has not translated into operational use.
Review costs on both sides: Count platform and engineering effort, then compare that with time saved, duplicate tooling reduced, and delivery cycles shortened.
For teams that want examples grounded in actual implementations, these healthcare client case studies can help compare how different organizations connected use cases to measurable results.
Choosing the Right Technology and Partner
A data fabric that looks polished in a demo can still fail the first time an auditor asks for lineage, a source schema changes overnight, or a clinical workflow depends on data arriving on time. Choosing the right platform means testing whether the fabric can hold under real operating pressure, not whether the interface looks modern.
The easiest way to evaluate a healthcare data fabric is to treat it like a fabric inspection before it goes into production. You do not just check the color and texture. You pull on the threads, look for weak joins, and see how it behaves after repeated use. In healthcare, those threads are standards support, metadata, policy enforcement, resilience, and the delivery model behind the technology.
What to evaluate first
Start with the parts that determine whether the platform will still be usable a year from now, after new data sources, new reporting demands, and new compliance reviews arrive.
Standards support: Can the platform work cleanly with HL7, FHIR, claims files, images, and semi-structured clinical content without forcing custom handling for every source?
Metadata depth: Can your team trace lineage, schema changes, data quality rules, and policy context in a form that engineers, analysts, and auditors can all use?
Access patterns: Can the same governed data serve APIs, event-driven workflows, dashboards, analytics notebooks, and application services?
Security controls: How are identity, role-based access, encryption, consent-related restrictions, and audit logging handled in production?
Scalability across domains: Can the architecture extend from one use case to another, such as from readmission analysis to prior authorization, without rebuilding the core model?
These questions matter because a healthcare data fabric is not just an integration layer. It becomes the operating weave between systems, policies, and people. If one thread is weak, the strain shows up everywhere else.
Vendor and Technology Evaluation Checklist
| Evaluation Criteria | Why It Matters | Key Questions to Ask |
|---|---|---|
| Standards interoperability | Healthcare environments run on mixed formats, legacy interfaces, and newer APIs | Which healthcare formats, message types, and APIs are supported with minimal custom work? |
| Metadata and lineage | Trust and auditability depend on clear traceability | Can we trace data from source through transformation to each application or report output? |
| Governance model | Distributed access only works if policy stays consistent | Where are policies defined, and how are they enforced across tools and teams? |
| Operational resilience | Clinical and financial workflows need dependable delivery | How are failures detected, escalated, recovered, and documented? |
| AI readiness | AI and analytics only work when data is governed and usable | How does the platform expose governed data to ML pipelines, vector stores, or analytical tools? |
| Delivery fit | A strong platform can still fail with the wrong implementation model | Which responsibilities belong to our internal team, and which can a partner handle credibly? |
Ask for evidence, not promises.
A useful vendor session should include more than architecture diagrams and feature lists. Ask them to walk through a schema change, a failed pipeline, a revoked user entitlement, and an audit request for lineage history. If they cannot show how the platform behaves under those conditions, you are still looking at marketing, not production readiness.
How to assess the partner, not just the product
The platform is only half the decision. The partner shapes whether the architecture is installed as a one-time project or built as an operating capability your team can sustain.
A strong partner in healthcare usually shows four traits. First, they understand clinical and payer workflows well enough to map technical design choices to operational consequences. Second, they can explain compliance controls in practical terms, including how access, retention, logging, and change management work after go-live. Third, they design for handoff, so your internal team is not permanently dependent on outside specialists. Fourth, they connect technical milestones to measurable business results such as shorter delivery cycles, less duplicate integration work, faster reporting turnaround, or cleaner data for care operations.
One useful test is simple. Ask the partner how they would validate the platform before calling it ready for production. An experienced team should describe control testing, lineage verification, failure scenarios, role review, and workflow-level acceptance criteria. If the answer stays at the level of generic cloud security claims, keep asking questions.
The right choice is the combination that fits your environment, your risk profile, and your operating model. In healthcare, a good decision is rarely the platform with the longest feature list. It is the one whose threads stay intact when compliance, integration complexity, and outcome measurement all pull at once.
Frequently Asked Questions About Healthcare Data Fabric
Is a healthcare data fabric the same as a data warehouse?
A healthcare data fabric and a data warehouse solve different problems.
A warehouse brings data into one repository, usually for reporting, analytics, and historical analysis. A data fabric works more like the threads that connect many systems into one usable layer. It coordinates access, metadata, lineage, and policy across distributed sources, whether the data stays in place or moves into downstream stores. In practice, many healthcare organizations use both. The warehouse remains one destination. The fabric provides the rules and connective tissue around it.
Can it work with legacy hospital systems?
Yes, but only if the design starts from the reality of your environment.
Hospitals rarely operate on clean, modern stacks alone. They run older EHR modules, departmental systems, batch feeds, flat files, and vendor-specific interfaces that were never designed to work together gracefully. A data fabric does not remove that complexity. It helps your team handle it with repeatable patterns for ingestion, transformation, metadata management, and governed access, so integration stops feeling like custom plumbing every time a new source appears.
Does a healthcare data fabric mean we no longer need integrations?
You still need integrations. What changes is how you build and govern them.
Without a fabric, each interface often becomes its own small project, with separate mapping logic, separate monitoring, and separate failure points. Over time, that creates a patchwork that is expensive to maintain and hard to audit. A fabric gives you shared services and standards, so new connections use common rules for ingestion, mapping, lineage, and access control. The result is less duplication and a clearer operating model.
How long does implementation take?
There is no honest universal timeline.
The duration depends less on product demos and more on the shape of your data estate, the quality of source contracts, the maturity of governance, and the number of legacy exceptions your team has to account for. A practical rollout is phased. Start with one use case that matters, such as quality reporting, prior authorization data exchange, or cross-system patient analytics. Validate operational behavior and control evidence there first. Then expand with patterns your team has already proven in production.
How do we validate compliance beyond vendor claims?
Treat compliance validation like a production readiness exercise, not a procurement checkbox.
Ask for evidence tied to your workflows and risk profile. Review how lineage is captured, how roles are designed and approved, how encryption works in transit and at rest, how audit logs are retained, how policy changes are documented, and how incidents are investigated. Then run a pilot that produces artifacts your compliance, security, and internal audit teams can inspect directly.
The critical question is whether your architecture can show, in a traceable way, who accessed what data, under which policy, through which workflow, and with what controls in place. That is the difference between a promising platform and an audit-ready operating model.
Can a healthcare data fabric support generative AI?
Yes. In many organizations, AI interest is what exposes the weakness of the current data foundation.
Generative AI depends on reliable, governed access to both structured and unstructured data. If clinical notes, claims files, imaging metadata, and operational records all live in disconnected silos, model outputs become harder to trust and harder to explain. A data fabric helps by creating a more consistent layer for discovery, policy enforcement, and traceability. That matters not only for model performance, but also for clinical review, privacy oversight, and downstream accountability.
How should we measure success in the first year?
Start with evidence that the data foundation is working. Then connect that evidence to business and care outcomes.
Useful first-year measures often include source onboarding time, reduction in manual data preparation, improvement in lineage visibility, fewer duplicate integration efforts, better reliability of data delivery, and faster turnaround for reporting or operational workflows. Once those indicators are stable, measure downstream impact such as fewer delays in care operations, cleaner quality reporting, faster financial reconciliation, or better support for utilization and population health programs.
Many initiatives lose credibility. They claim clinical or financial improvement before proving that the data path is trusted. A stronger approach is to show the chain of evidence from governed data access to workflow improvement to measurable outcomes.
About Upendra Jith
Upendrajith completed his Master's in English and has been a commercial content developer for the past three years. He's more inclined to develop content with a 'street-smart' delivery on topics such as technology, media, or anything he can get his hands on. He has a fixation on lyrics, dark poetry, media, technology, and flow arts.
View all posts by Upendra Jith →