


Healthcare Digital Twins: AI & ROI for Healthtech
Healthcare digital twins have moved out of the innovation lab and into board-level planning. The clearest signal is market momentum. The global healthcare digital twins market was valued at USD 902.6 million in 2024 and is projected to reach USD 3.55 billion by 2030, growing at a 25.9% CAGR, according to Grand View Research's healthcare digital twins market analysis.
That matters because this isn't just another AI buzz cycle. Health systems, medtech companies, and healthtech SaaS teams are now treating healthcare digital twins as a practical way to model patient risk, test treatment pathways, and improve operational decisions before they affect real people.
The opportunity is real. So are the traps. The integration burden is often underestimated, model readiness is overestimated, and bias and governance questions are left until late. That's the wrong order.
The Unstoppable Rise of Healthcare Digital Twins
A market growing at 25.9% a year gets board attention for a reason. Healthcare digital twins are moving into serious product and operations planning because leaders want better decisions before they commit clinical, operational, or financial resources.
For CTOs, the strategic question is no longer whether the concept is interesting. It is whether your organization can turn it into a dependable capability. That depends less on demo quality and more on execution. Legacy EHRs, inconsistent HL7 and FHIR implementations, fragmented imaging systems, and weak master data practices will slow or sink a digital twin initiative long before model design becomes the limiting factor.
That is why the rise of healthcare digital twins matters. They shift software from reporting and prediction into simulation and intervention testing. In practice, that means a health system can model patient deterioration risk, stress-test care pathways, or simulate bed capacity and staffing decisions before those choices affect real patients.
The opportunity is real. So is the failure rate for teams that treat this as an AI feature instead of a cross-functional platform investment.
Why the timing matters
Buyer interest is rising because healthcare organizations are under pressure to improve outcomes and efficiency at the same time. A digital twin supports that goal only if it can absorb live data from the systems that run care. In many environments, that is the hard part. Data sits across EHR modules, labs, PACS, device feeds, claims systems, and spreadsheets maintained outside formal governance.
If you cannot reconcile identities, normalize events, and maintain a reliable update loop, you do not have a digital twin. You have a disconnected model with stale inputs.
That distinction matters for investment decisions. Teams building for precision medicine, remote monitoring, oncology workflows, device analytics, or hospital operations should evaluate digital twins now, but they should do it with strict entry criteria:
-
Interoperability first: Audit your HL7, FHIR, DICOM, device, and data warehouse readiness before funding model work.
-
Bias controls early: Test for representation gaps and skewed outputs before any clinical workflow depends on the system.
-
Governance by design: Set rules for data lineage, versioning, validation, and human oversight at the start.
-
Narrow initial scope: Begin with one high-value use case where data quality is strong enough to support continuous updating.
What separates this from generic healthcare AI
Generic healthcare AI usually classifies, summarizes, or predicts. A digital twin maintains a current representation of a patient, device, or care environment and uses that model to test scenarios.
That difference changes the standard for what you need to build.
-
A prediction model tells you what may happen next.
-
A digital twin helps you compare what may happen under different interventions, constraints, or operating conditions.
That is a stronger business case, but it comes with stricter requirements. The model has to stay aligned with reality. The data pipeline has to handle drift, missing values, and latency. Clinical leaders need visibility into how recommendations are produced. Compliance teams need traceability. If algorithmic bias is discovered late, remediation gets expensive, and trust drops fast.
Healthcare digital twins create value when they support real decisions under real constraints, not when they stay trapped in a polished pilot.
Treat this as decision infrastructure. Build only where interoperability is achievable, governance is enforced, and bias monitoring is active from day one. That is how digital twins move from industry hype to durable healthtech advantage.
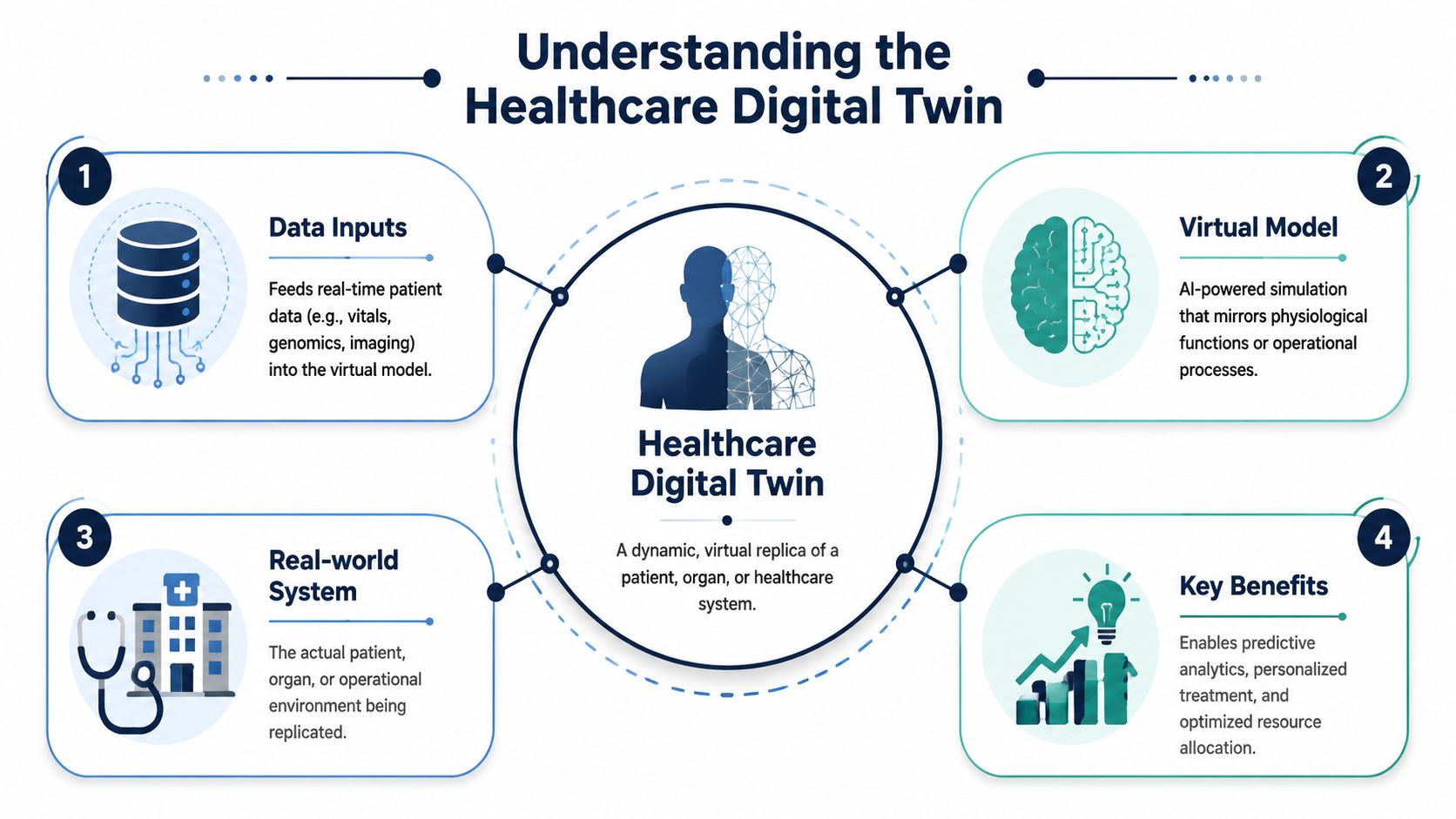
What Exactly Is a Healthcare Digital Twin
Most explanations are too abstract. Here's the practical version. A healthcare digital twin is a continuously updated simulation of a real patient, organ, device, or hospital system that uses incoming data to reflect current conditions and estimate likely outcomes.
A good analogy is a flight simulator. Pilots don't use it because it looks realistic. They use it because it lets them test conditions, rehearse responses, and reduce risk before the live event. That's what a digital twin does in healthcare.
A healthcare digital twin is a virtual model that stays connected to the real-world entity it represents and improves decisions through simulation.
The three parts that actually matter
A working twin usually depends on three layers.
The data model
This is the representation of its physical subject. For a patient, that may include medical history, imaging, lab results, medication patterns, wearable data, and disease-specific variables. For a hospital, it may include admissions flow, staffing behavior, equipment utilization, and bed capacity.
The key point is fidelity. If the model only reflects fragments of reality, the twin becomes an expensive visualization tool, not a trustworthy simulation environment.
The simulation engine
Value is created when the engine interprets incoming data, applies analytical or machine learning logic, and projects how the system may behave under different conditions.
Clinical-grade digital twins integrate real-time data from EHRs, wearable IoT sensors, and high-resolution imaging into a dynamic simulation model. That continuous feedback loop creates a cause-and-effect relationship between biometric data and predicted disease progression, which is a major step beyond static models.
The feedback loop
A twin without feedback is just a snapshot. The feedback loop is what keeps the model aligned with reality. New vitals, updated imaging, changing medication adherence, or new operational constraints should influence the model continuously.
What a healthcare digital twin is not
A lot of products are being labeled as digital twins when they aren't.
| Tool type | What it does | Why it isn't a true twin |
|---|---|---|
| Dashboard | Displays status and KPIs | It reports. It doesn't simulate. |
| Risk score model | Predicts a narrow outcome | It predicts one thing, not system behavior. |
| Rules engine | Triggers actions from thresholds | It reacts to conditions but doesn't model state changes. |
| Static 3D model | Visualizes anatomy or assets | It looks detailed but doesn't learn from live data. |
Where this definition becomes useful
Once you define the twin properly, product decisions get sharper. You can decide whether you're building:
-
A patient twin for treatment planning
-
An organ twin for disease-specific simulation
-
An operational twin for hospital flow and capacity management
-
A hybrid SaaS layer that combines multiple twin types
If your roadmap includes custom healthcare software development, this distinction matters early. It affects your data contracts, modeling scope, clinical validation path, and commercial positioning.
Transformative Use Cases in Clinical and Operational Settings
The value of healthcare digital twins becomes obvious when you look at where they help people make better decisions. The strongest use cases fall into two camps. Clinical care and operational execution.

Clinical use cases that justify the complexity
Oncology is one of the clearest examples. According to Stanford Medicine's report on medical digital twins, AI-powered medical digital twins can model tumor growth and predict chemotherapy response with high accuracy, allowing clinicians to simulate treatment paths and reduce adverse outcomes by identifying non-responsive therapies before treatment proceeds.
That's a serious shift in care logic. Instead of committing to a therapy and watching what happens, teams can test the likely response inside the model first.
Other high-value clinical scenarios follow the same pattern:
-
Personalized treatment planning: The twin helps compare therapeutic options against a patient-specific profile.
-
Disease progression monitoring: The system updates as new signals come in, which supports earlier intervention.
-
Pre-procedure simulation: Clinicians can evaluate likely outcomes before acting on patients.
A related capability that often gets overlooked is document intelligence. Before a twin can reason well, it needs a usable clinical context. Teams evaluating ingestion and interpretation pipelines should also discover AI solutions for healthcare records, especially when records arrive as fragmented PDFs, scans, and mixed-format medical documents.
Operational use cases that pay off faster
Not every digital twin should start with a patient. In many organizations, the better first move is an operational twin.
Hospitals and provider networks can model patient pathways, staffing behavior, and resource constraints to spot bottlenecks before they damage care delivery. A simulation can test what happens when admissions rise, capacity shifts, or scheduling patterns change. That makes workforce and throughput decisions more deliberate.
Start where the feedback loop is fastest. Operational twins often reach usable value sooner than full patient twins.
The pharmaceutical side also matters. Verified industry material notes that Takeda Pharmaceuticals used digital twin simulations to optimize drug development processes by virtually testing treatment options on simulated organ systems before human trials. The point isn't the brand name. The point is the pattern. Simulation shortens the loop between hypothesis and decision.
Where teams should focus first
If you're building a healthtech platform, don't try to launch every twin concept at once. Pick one use case with three traits:
-
Clear decision impact
-
Accessible data inputs
-
A buyer who already feels the pain
That's also where the SaaS product development discipline matters. A digital twin product isn't just an AI model. It's a workflow product with clinical stakes, UX requirements, integration demands, and audit expectations.
The Technology Stack and Architecture Requirements
Digital twin programs usually break at the integration layer, not the model layer. The idea is attractive. The hard part is getting messy clinical, operational, and device data into a system that can update reliably, explain its outputs, and survive audit scrutiny.
The four layers you need to design properly
A healthcare digital twin needs four layers working together. If one layer is weak, the twin becomes a demo instead of a production system.
Data acquisition
Start with the source systems you already have, not the sources you wish you had. That usually means EHRs, imaging systems, labs, bedside devices, claims feeds, and wearables. The ingestion problem is not volume alone. It is late feeds, missing fields, inconsistent timestamps, and patient identity mismatches across legacy platforms.
A twin only stays useful if the underlying state stays current. If updates arrive in batches once or twice a day, your model will lag behind the clinical reality it is supposed to represent.
Integration and interoperability
This layer decides whether your program scales or stalls. Healthcare data lives in siloed products, old interfaces, vendor-specific schemas, and partially implemented standards. FHIR helps, but it does not fix poor source quality, broken terminology mapping, or conflicting identifiers.
Your architecture needs normalized pipelines, terminology management, master data strategy, API governance, and event handling. You also need a clear answer to a basic question: does the twin read directly from source systems, consume curated data products, or run on top of a governed data platform? For most organizations, the middle option is the safest. It reduces production risk, improves traceability, and gives data engineering teams room to clean and validate inputs before models use them.
Teams that lack this foundation should build it first through data and AI engineering services. Fancy simulation on top of weak interoperability is a waste of budget.
AI and simulation
This is the decision layer. In practice, it is rarely one model. A serious twin may combine rules, time-series forecasting, probabilistic inference, optimization, and simulation logic in the same workflow.
The bigger risk is not technical complexity alone. It is bias hidden inside the training data and model assumptions. If your data mainly reflects one patient population, one care pathway, or one hospital network, your twin can produce confident recommendations that fail for underrepresented groups. That is an architecture issue, not just an ethics issue. You need model monitoring, cohort-based validation, version control, and a review process that catches performance gaps before they affect care or operations.
The application layer
Trust is won or lost.
Clinicians, operators, and care managers need interfaces that show what changed, which inputs drove the output, what level of confidence the system assigns, and what action is recommended. Add audit logs, role-based access, and workflow-specific views from the start. If users have to leave their existing systems to interpret a black-box prediction, adoption will drop fast.
Architecture decisions that deserve executive attention
CTOs should force early decisions on a few points that teams often postpone:
-
System of record: Define where the twin state lives and how it syncs with source systems.
-
Update model: Choose event-driven, scheduled, or hybrid updates based on the use case and data latency tolerance.
-
Identity resolution: Set rules for matching patient, device, and encounter data across fragmented systems.
-
Validation: Test outputs at both the model level and workflow level, because accurate predictions can still fail in real operations.
-
Conflict handling: Decide which source wins when records disagree, and assign human review for unresolved anomalies.
-
Bias controls: Require subgroup testing and retraining triggers, not just aggregate accuracy reports.
Build for data trust first. Then improve model sophistication.
That order matters in healthcare more than in almost any other sector. If your current stack cannot support governed pipelines, interoperable data products, explainable outputs, and repeatable validation, you are not ready for a high-stakes digital twin deployment. Start with the plumbing, especially in environments dominated by legacy systems. That is where the core implementation work is.
Navigating Regulatory Compliance and Ethical Considerations
Most digital twin discussions spend too much time on innovation theater and not enough time on exposure. In healthcare, a twin can influence treatment, prioritization, and operational decisions. That means privacy, traceability, consent, and fairness aren't side topics. They're core design constraints.
Consent and governance are product requirements
A digital twin depends on broad, continuous data usage. That changes the governance burden. It's not enough to secure data at rest and in transit. Teams also need clear policies for data provenance, access control, model updates, retention, auditability, and clinician oversight.
Siemens Healthineers defines four prerequisites for healthcare digital twin implementation: hospitals must be digitally networked, data must be structured and annotated with clinical metadata, patients must retain full decision-making authority over data usage, and medical professionals must have real-time access to the digital interface, according to its digital patient twin perspective. That's a practical baseline, not an aspirational ideal.
Bias is the harder issue
The more neglected problem is algorithmic bias. Many digital twin models are trained on data from Western populations, which can produce biased or ineffective predictions for patients in African, Asian, or Latin American regions, as highlighted in this OUP analysis on digital twins and health equity.
That creates a serious leadership question. If your model performs well in London but poorly in Nairobi, you don't have a globally valid product. You have a regional model with international branding.
A credible response requires more than a disclaimer:
-
Audit training data coverage: Know which populations are represented and which aren't.
-
Test outputs across demographic slices: Don't settle for aggregate performance.
-
Localize validation: Review model behavior with regional clinical input.
-
Set escalation rules: High-risk outputs should trigger human review, not silent automation.
If your bias mitigation plan starts after launch, you're already behind.
Compliance should shape architecture early
CTOs often ask whether they should solve product fit first and compliance later. In healthcare digital twins, that sequencing causes rework. Consent handling, audit trails, explainability hooks, and access boundaries should be built into system design from the start.
That's especially true when AI components affect regulated workflows. Teams that need a deeper view of policy, risk, and technical controls should review guidance on AI regulatory compliance and security for medtech. It's easier to design for auditability early than to retrofit it under pressure.
An Implementation Roadmap for Your Digital Twin Initiative
Most healthcare digital twin initiatives fail in the planning stage while everyone pretends they're progressing. The slide deck looks polished. The architecture diagram looks modern. Then the team discovers the records are fragmented, source systems disagree, and data cleaning consumes the schedule.
That's why implementation should start with constraints, not ambition.
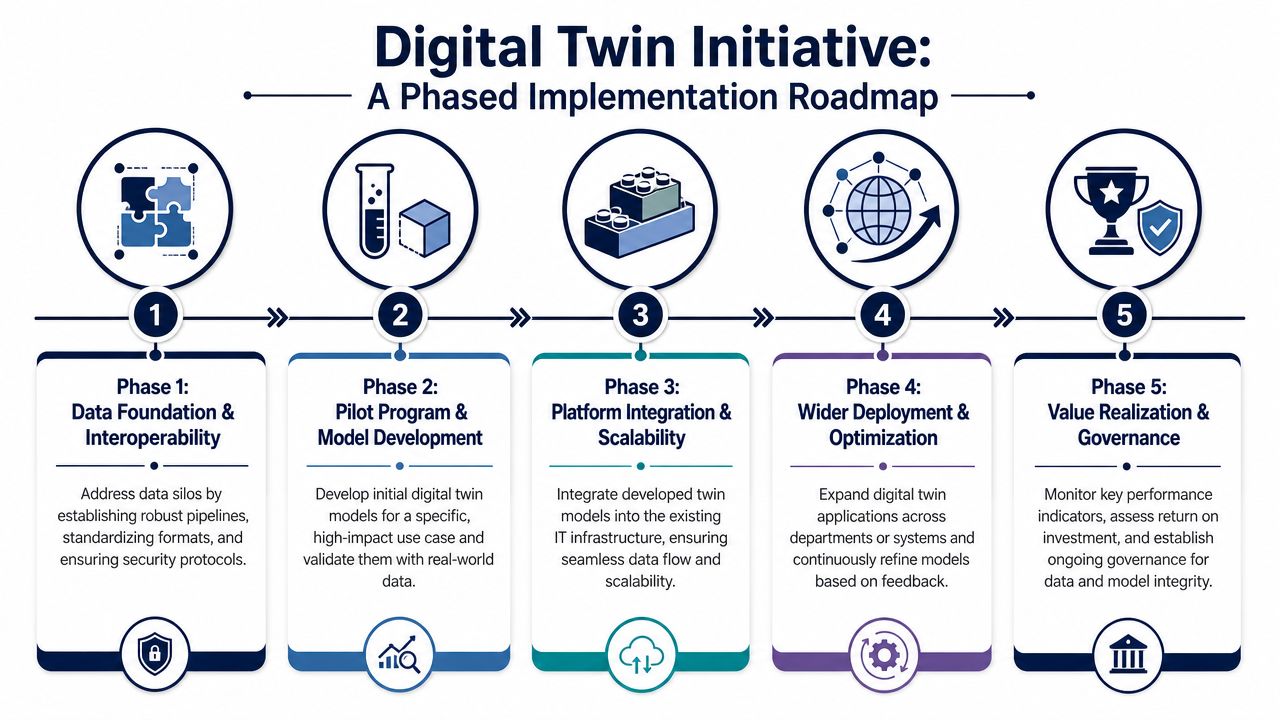
Phase 1 builds the foundation
A major barrier is the data interoperability nightmare created by fragmented, non-standardized EHRs. Projects can face a 40 to 60 percent timeline increase due to custom data cleaning, according to the cited interoperability review on PMC. If your records span multiple legacy systems, old ERP layers, and inconsistent clinical vocabularies, this is your first problem, not model selection.
Start with a hard readiness assessment:
| Question | Why it matters |
|---|---|
| Are core systems digitally networked? | Without connected systems, the twin won't stay current. |
| Is clinical data structured and annotated? | Unstructured ambiguity limits simulation quality. |
| Can patients control data usage decisions? | Governance failures can block deployment. |
| Do clinicians have real-time interface access? | A twin no one can use is irrelevant. |
Those four checks mirror the Siemens prerequisites referenced earlier. If you fail two or more, don’t move into full product development yet.
Phase 2 chooses the right pilot
Pick a narrow use case with real operational or clinical pain. Don’t begin with the broadest vision. Start with a use case where data is available, workflows are visible, and outcomes can be reviewed by domain experts.
Good first pilots usually have these traits:
-
Bounded scope: One service line, one disease area, or one operational bottleneck.
-
Measurable workflow value: The pilot should influence actual decisions.
-
Available reviewers: Clinicians or operations leaders must validate outputs continuously.
Phase 3 develops an MVP that can survive scrutiny
Many teams confuse a prototype with a product. A demo can impress stakeholders. An MVP for healthcare must survive review, logging, exception handling, and data quality issues.
Build for controlled use first:
-
Connect limited but trusted data sources
-
Implement core simulation logic
-
Create a reviewable interface
-
Log every output and override
-
Validate with domain users before scaling
If you need a structured sequence for that work, an AI implementation roadmap is more useful than a generic innovation workshop because it forces decisions around readiness, risk, and execution order.
For teams still deciding how to organize delivery, different software development service models can fit different realities. A startup building a new twin-enabled platform may need one model. A provider retrofitting existing systems through custom software development may need another provider.
Phase 4 and Phase 5 scale with discipline
Once the pilot works, expand through governed repetition, not uncontrolled enthusiasm. Reuse patterns for integration, validation, role-based access, and monitoring.
Also, get serious about AI policy before scale. Teams that need a grounded external read on the policy side should look at navigating AI compliance. It’s a useful companion to the architectural work because governance gaps usually widen during rollout.
Build one trustworthy twin before you promise a twin ecosystem.
Measuring the True ROI of Digital Twin Investments
Analysts at Nature Medicine found positive results in 36 of 45 measured outcomes, or about 80% overall effectiveness, across digital twin applications in precision health management, according to this review of digital twin effectiveness. That is enough evidence to take the category seriously. It is not enough to fund a twin program on faith.
A healthcare digital twin earns its budget only when it improves a decision, changes an action, and produces an outcome your finance, clinical, or operations leaders can verify. If the model looks impressive but the staff ignores it, you built an expensive demo. If the model gets used but cannot be connected to workflow, audit trails, or legacy systems, you built technical debt with better branding.
Measure ROI in three layers.
First, measure adoption inside the workflow. Track recommendation acceptance, override rates, time to action, and whether the twin changes care planning, scheduling, capacity allocation, or device maintenance decisions.
Second, measure operational and clinical effect. Focus on metrics tied to the original use case, such as lower length of stay, fewer avoidable escalations, better resource utilization, faster planning cycles, or reduced readmission risk. Pick a short list and tie every metric to a baseline.
Third, measure implementation drag. Many business cases collapse at this point. If your team spends months cleaning fragmented EHR data, mapping incompatible terminologies, and building interfaces into brittle legacy systems, the model may perform well while the program still underdelivers financially. Include integration cost, validation effort, governance overhead, and retraining work in the ROI model from day one.
Bias and trust belong in the ROI discussion, too. A twin that performs unevenly across patient groups creates clinical risk, review burden, and potential regulatory exposure. That cost is real. Add fairness testing, exception review, and model monitoring to the business case instead of treating them as side tasks.
Market growth projections and executive interest support the direction of travel, but they do not prove your return. Your return comes from tighter workflows, fewer avoidable mistakes, and better use of constrained staff and assets. It also depends on whether your architecture can support the twin without constant manual repair.
The smartest teams use stage-gated ROI targets. They do not ask a pilot to justify an enterprise platform. They ask it to prove one decision loop, one integration pattern, and one measurable improvement. Then they expand.
If you want a grounded benchmark for what healthcare software delivery looks like outside slide decks, review these healthcare client case studies. Use them to compare delivery realities, not to skip your own ROI discipline.
Frequently Asked Questions About Healthcare Digital Twins
Are healthcare digital twins only useful for large hospital systems?
No. Mid-sized healthtech startups and specialized providers can benefit, especially when they target a narrow problem. A twin for oncology treatment support, remote monitoring, or patient flow in one department is more realistic than an enterprise-wide twin from day one.
What’s the best first use case?
Start where the data is available, and the decision loop is clear. Operational bottlenecks, treatment pathway support, and disease-specific monitoring are usually better entry points than a broad “digital patient” vision. The first win should prove trust and workflow value.
Do you need real-time data for a digital twin to work?
Not always in the strictest sense, but you do need timely updates that match the decision context. A critical care use case needs fresher data than a longer-horizon planning model. The mistake is assuming “real-time” is mandatory everywhere or optional everywhere. It depends on the clinical or operational consequence.
How long does implementation take?
There’s no honest universal answer because legacy complexity dominates the schedule. If your organization has fragmented EHRs, inconsistent terminology, and brittle interfaces, integration work will take longer than model experimentation. That’s why data readiness should be assessed before committing to aggressive launch dates.
What makes a digital twin different from a predictive model?
A predictive model usually estimates one outcome. A digital twin represents an evolving system and can simulate how that system behaves under different interventions or conditions. It’s broader, more stateful, and more dependent on reliable feedback loops.
Is algorithmic bias really a practical concern for startups?
Yes. If your training data doesn’t represent the populations you serve, performance can break in clinical practice. That creates clinical, commercial, and regulatory exposure. Bias review isn’t something you add after product-market fit. It belongs to validation from the beginning.
Can a digital twin be delivered as a SaaS product?
Yes, but only if the product handles integration, governance, explainability, and tenant-specific variability well. In healthtech, SaaS doesn’t remove complexity. It packages complexity. The architecture still has to support compliance and clinical trust.
What should a CTO ask before approving a digital twin initiative?
Ask five things:
-
What exact decision will this twin improve
-
Which systems provide the data
-
How will outputs be validated
-
Who owns governance and clinical review
-
What happens when the model is wrong
If your team can’t answer those clearly, you’re not ready to scale.
Bridge Global helps healthtech teams turn complex AI ideas into compliant, production-ready platforms. If you’re planning a digital twin initiative and need a partner for architecture, interoperability, AI engineering, or scalable product delivery, explore Bridge Global as your healthtech software development partner. You can also review its healthcare expertise in custom healthcare software development, broader enterprise AI solutions, and proven client cases.
About Upendra Jith
Upendrajith completed his Master's in English and has been a commercial content developer for the past three years. He's more inclined to develop content with a 'street-smart' delivery on topics such as technology, media, or anything he can get his hands on. He has a fixation on lyrics, dark poetry, media, technology, and flow arts.
View all posts by Upendra Jith →