


Healthcare Cloud Migration: A Step-by-Step Playbook
Healthcare cloud migration isn't a niche modernization project anymore. The global healthcare cloud migration services market is valued at US$ 2,624.3 million in 2024 and projected to reach US$ 12,650.5 million by 2030, a 30.9% CAGR, according to Grand View Research. That growth matters because it changes how hospital leaders should think about migration. This is no longer just an infrastructure refresh. It's the foundation for resilience, interoperability, and future AI use.
The mistake I still see most often is treating healthcare cloud migration as a server move. Lift the workloads, recreate the network, cut over, and declare victory. That approach may reduce some hosting pain, but it usually leaves the hospital with the same operational friction, the same data quality issues, and the same compliance blind spots, just running in someone else's data center.
A first major migration needs a different mindset. The right goal isn't “get to cloud.” The right goal is to build a cloud environment that can safely support clinical operations today and advanced analytics, automation, and AI tomorrow. That means strategy first, compliance by design, disciplined data work, phased execution, and strong Day 2 operations.
Building Your Strategic Foundation for Cloud Migration
A migration without a business case usually turns into a technical program with no durable executive support. In healthcare, that's dangerous because the hard decisions arrive early. Which systems move first. Which dependencies stay on-premises. Which workflows can tolerate change. If leadership hasn't agreed on the why, the project stalls the first time clinical risk or budget pressure appears.
The strongest business cases tie cloud decisions to operational outcomes. Cost still matters. In fact, cost reduction is the top expected benefit for 74% of healthcare organizations, followed by improved operational efficiency at 50% and scalability at 42%, based on the cited findings in this industry summary. But a hospital CTO should frame migration more broadly than savings alone. The cloud should improve disaster recovery posture, support telehealth elasticity, simplify integration work, and create a cleaner path for analytics and AI.
Start with application and dependency truth
Most hospitals underestimate their own environment. They know the major systems. They often don't know the hidden connectors, the flat-file transfers, the departmental apps running on old virtual machines, or the reporting jobs that break if one table name changes.
Build an inventory in layers:
-
Clinical core systems such as EHR, PACS, LIS, RIS, and patient portals
-
Departmental applications including scheduling, pharmacy, revenue cycle, and specialty tools
-
Interfaces and dependencies such as HL7 feeds, FHIR APIs, SFTP jobs, identity flows, and third-party integrations
-
Data assets including structured records, imaging archives, logs, audit trails, and research datasets
That inventory isn't paperwork. It tells you what can be rehosted, what needs replatforming, and what shouldn't move until it's redesigned.
Practical rule: If you can't map a system's upstream and downstream dependencies, you're not ready to schedule its migration window.
Define success in operational terms
Good KPIs for healthcare cloud migration aren't generic infrastructure metrics alone. Uptime and backup success matter, but they don't tell a CTO whether the move improved care delivery. Tie migration success to clinical continuity, interface stability, release velocity, reporting reliability, and turnaround time for operational insights.
For a useful outside perspective on sequencing and executive alignment, Kogifi's piece on planning your enterprise cloud move is worth reading. It aligns with what works in practice. Strategy has to come before platform selection.
A practical assessment should also separate workloads into categories:
| Workload type | Typical migration posture | What to watch |
|---|---|---|
| Stable legacy apps | Rehost or contain | Hidden dependencies and unsupported OS/runtime |
| Integration-heavy systems | Replatform selectively | Message transformation, latency, interface testing |
| Data platforms | Modernize deliberately | Governance, lineage, retention, access controls |
| Innovation workloads | Build cloud-native | Cost controls, security boundaries, service eligibility |
Build the case stakeholders will actually support
The CFO wants predictability. Clinical leaders want low disruption. Security wants auditability. Operations wants fewer outages. Your migration narrative has to satisfy all four.
That's where an experienced healthtech software development partner can help pressure-test assumptions against real client cases. It also helps to ground strategy in architecture considerations specific to providers, such as those discussed in cloud infrastructure for healthcare systems.
Don't ask the board to approve “cloud migration.” Ask them to approve a staged program that reduces operational risk, modernizes critical integration points, and prepares the organization for secure AI adoption.
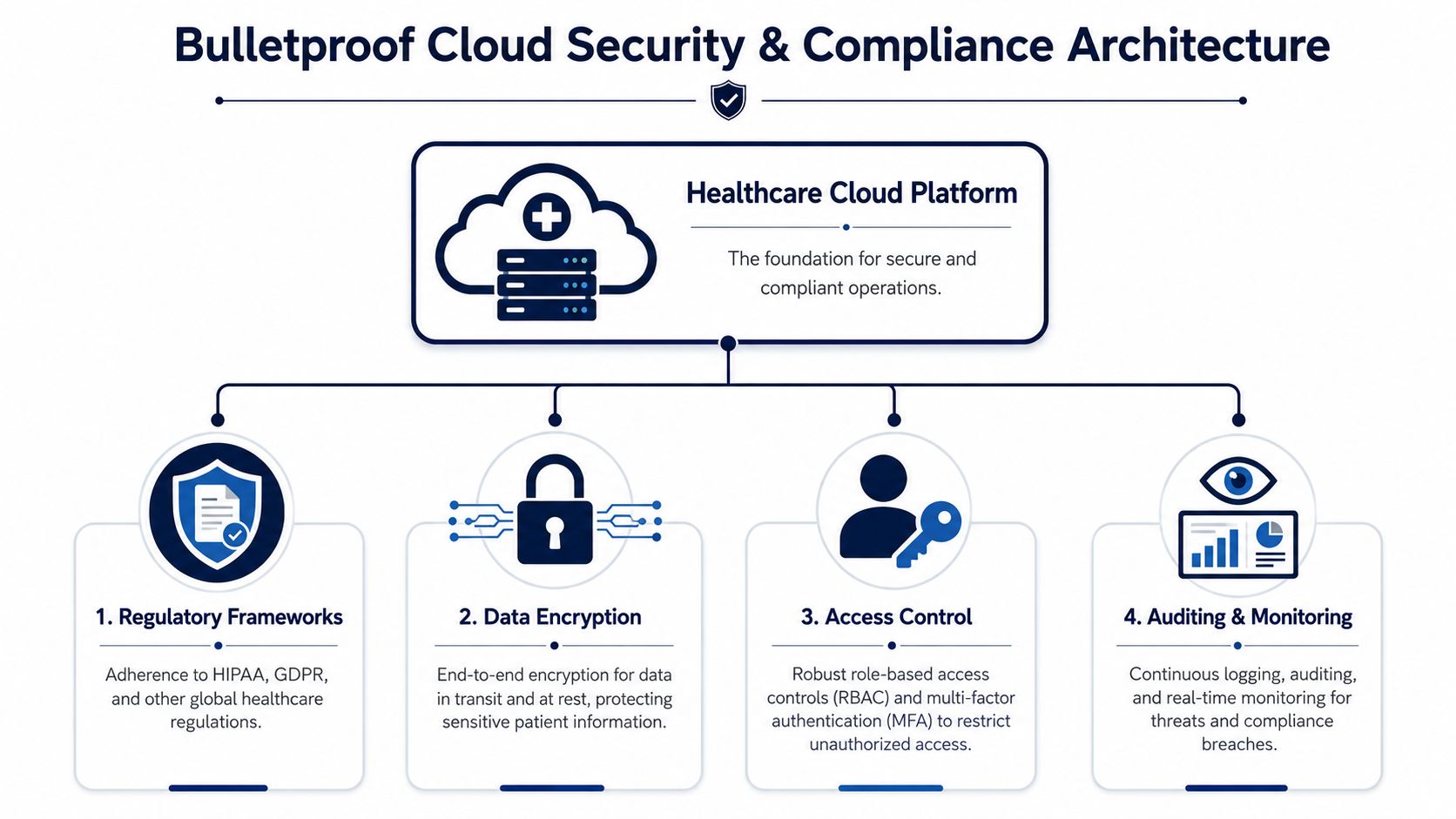
Architecting for Bulletproof Security and Compliance
In healthcare, compliance can't be bolted on after the landing zone is built. If your security model, service selection, and audit controls aren't part of the initial architecture, you'll spend the rest of the program remediating preventable mistakes. That's more expensive, slower, and riskier than designing correctly from day one.
The legal trigger is straightforward and often mishandled. Organizations must execute signed Business Associate Agreements with every cloud provider receiving ePHI and confirm that specific services used appear on the provider's HIPAA-eligible list to maintain compliance under 45 CFR §164.308(a)(1), as outlined in this HIPAA cloud migration guidance. Teams sometimes assume that using a major cloud vendor automatically solves this. It doesn't. Eligibility is service-specific, and your responsibility doesn't disappear because the infrastructure is managed.
The architecture has to reflect shared responsibility
Public cloud platforms secure the underlying platform. Your team still owns identity, access design, workload configuration, encryption choices, logging coverage, service usage, and data handling patterns. That's why “HIPAA-capable” marketing language is never enough.
A secure healthcare cloud architecture should include:
-
Identity as the primary control plane with role-based access control, least privilege, MFA, and strong separation between admin and clinical user paths
-
Encryption decisions made up front for data at rest, in transit, backups, and key management boundaries
-
Network segmentation that isolates sensitive workloads, management planes, and integration endpoints
-
Centralized audit logging across compute, storage, IAM, databases, and application layers
A useful supplemental read is Nutmeg Technologies' overview of HIPAA-compliant solutions. It's helpful because it reinforces the practical reality that compliance is operational, not declarative.
Hybrid and multi-cloud can help, but only if you govern them tightly
Some hospitals need hybrid patterns for latency, legacy imaging systems, or vendor constraints. Others use multi-cloud to reduce concentration risk or support specific analytics tools. Those choices can be valid. They also expand your control surface.
If you're mixing environments, define these before any workload moves:
| Control area | Question to settle early |
|---|---|
| Identity | Is there one authoritative identity model across environments |
| Logging | Can security teams search events across all platforms |
| Encryption | Who controls keys, and where are boundaries enforced |
| Data movement | Which routes are approved for ePHI transfers |
| Service approval | Who validates HIPAA eligibility for each service used |
Compliance failures rarely come from one dramatic design flaw. They usually come from a chain of small assumptions that nobody documented.
Treat policy and engineering as one workflow
Security teams often write policies after engineers have already built the landing zone. In healthcare, that sequence creates drift almost immediately. Architecture review, control mapping, IaC standards, service approval, and audit evidence collection need to run together.
That's also why governance content should sit close to architecture work. A practical reference is this guide to healthcare data governance. Governance is what turns a nominally compliant environment into one that survives audits, staff turnover, and new use cases.
A bulletproof design isn't the one with the most controls. It's the one where each control is mapped to an actual risk, implemented consistently, and tested before the first production dataset moves.
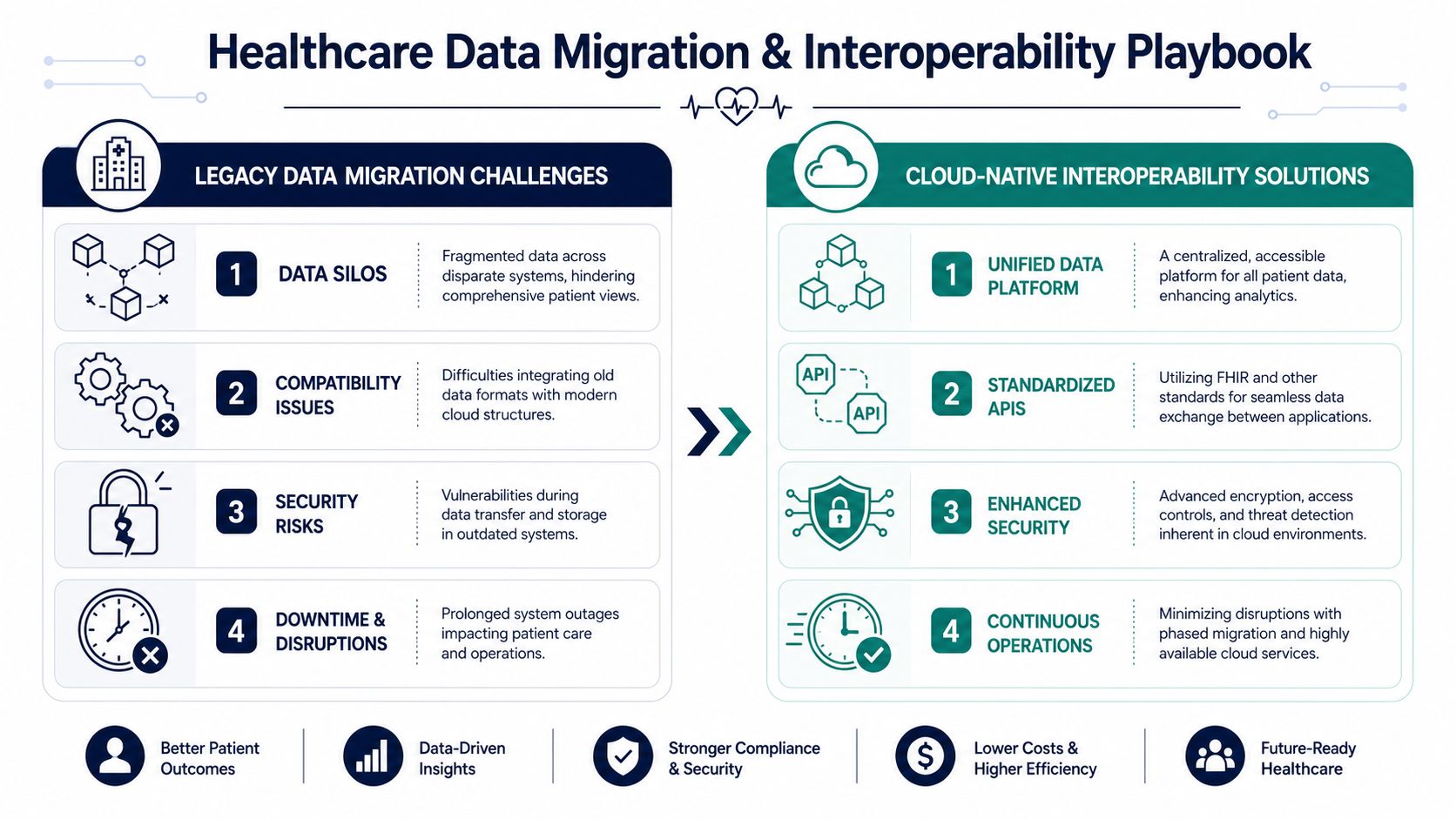
Executing Data Migration and Ensuring Interoperability
Data is where healthcare cloud migration succeeds or fails. Servers can be rebuilt. Containers can be redeployed. Broken patient identity, malformed clinical messages, and incomplete historical data create damage that's much harder to unwind.
The pattern behind many failed migrations is consistent. The most common migration failures stem from inadequate pre-migration data cleanup, missing HL7/FHIR interoperability mapping, and treating compliance as an afterthought rather than a core design principle. That matches what technical teams run into on the ground. The migration plan looks clean until dirty data, undocumented interfaces, and edge-case workflows hit the test environment.
Clean the data before you move it
Hospitals often try to migrate first and normalize later. That usually multiplies the effort. You end up paying to transfer duplicates, obsolete records, inconsistent coding patterns, and malformed fields into the new environment, then paying again to fix them.
The better sequence is:
-
Profile the source data to identify duplication, null-heavy fields, invalid formats, and coding inconsistencies
-
Define canonical structures for patient, encounter, provider, order, and result data before transformation begins
-
Tag records by migration treatment such as migrate, archive, transform, or exclude
-
Run sample migrations with reconciliation checks before touching production cutover waves
This is especially important for EHR extracts, claims data, imaging metadata, and research datasets where field-level quality issues can cascade into reporting and care workflows.
Interoperability isn't a side task
A surprising number of cloud programs still handle interoperability as interface cleanup to be tackled near go-live. In practice, HL7 and FHIR mapping should drive design decisions much earlier because they shape data contracts, transformation logic, and testing.
A sound interoperability workstream usually includes:
-
Current-state interface mapping across HL7 v2 feeds, FHIR endpoints, file transfers, and vendor APIs
-
Message-by-message validation for ADT, orders, results, scheduling, billing, and identity workflows
-
Canonical API design where cloud-native services expose standardized payloads rather than reproducing every legacy quirk
-
Operational monitoring for failed messages, latency spikes, duplicates, and schema drift
A migration is only “done” when downstream systems receive the right clinical data in the right format at the right time.
Strong healthcare integrations work matters because cloud platforms amplify both good and bad data patterns. If your integration design is disciplined, the cloud gives you cleaner interoperability and better analytics. If it isn't, the cloud helps broken interfaces fail faster.
Choose your migration pattern around clinical risk
A big-bang data cutover can work for narrow, low-risk systems. It's rarely the right move for core clinical platforms. Phased or trickle migration gives teams more control over validation, fallback, and workflow continuity.
A practical comparison looks like this:
| Migration pattern | Best fit | Main trade-off |
|---|---|---|
| Big bang | Small, contained systems | Higher cutover risk |
| Phased by department | Clinical environments with varied workflows | Longer coexistence period |
| Phased by data domain | Analytics and longitudinal records | More transformation planning |
| Trickle sync | Systems needing continuity during transition | More temporary integration overhead |
You'll also want a dedicated architecture for pipelines, not a collection of ad hoc scripts. Modern data engineering patterns are particularly important. If your team is redesigning ingestion and transformation paths, this piece on healthcare data pipeline architecture is a useful companion to migration planning.
The practical objective isn't to move all data quickly. It's to move the right data safely, preserve meaning, and leave the target environment cleaner than the source.
The Migration and Validation Playbook
Execution should feel controlled, boring, and heavily documented. If the migration phase feels improvisational, your planning was too shallow. The safest programs move in measured waves, with clinical leaders involved in each checkpoint and rollback criteria agreed before any change window opens.
A phased pilot is the pattern I'd recommend for a first major healthcare cloud migration. Migrations that adopt a phased, department-specific pilot approach achieve significantly higher success rates by validating clinical outcomes before full rollout, often requiring 12–18 months of meticulous planning. The planning time can frustrate impatient sponsors, but it's usually what prevents avoidable disruption later.
Pick the right migration motion for each workload
The classic “6 R's” framework is still useful if you apply it with discipline:
-
Rehost for stable workloads that need infrastructure relief but not architectural change yet
-
Replatform when the app can benefit from managed databases, storage, or runtime changes without code rewrite
-
Refactor for systems that need cloud-native resilience, better scaling, or API-first redesign
-
Retain when a workload has regulatory, vendor, or timing reasons to stay put
-
Retire when you discover duplicate or obsolete systems during the inventory phase
-
Repurchase when a SaaS replacement makes more sense than carrying a custom legacy footprint
For some hospital-adjacent products, especially digital front doors or operational apps, this can also lead into a broader SaaS product development model instead of a straight infrastructure migration.
Run the pilot where the blast radius is manageable
The first pilot shouldn't be your most politically visible department. It should be a clinically meaningful area with engaged leadership, manageable workflow complexity, and measurable outcomes.
Use a simple readiness screen:
| Phase (Duration) | Key Activities | Primary Roles Involved |
|---|---|---|
| Discovery and planning | Dependency mapping, risk review, success criteria, rollback design | CTO, enterprise architect, clinical leaders, security lead |
| Pilot preparation | Environment build, interface setup, data sampling, test plan definition | Cloud architect, integration engineer, data engineer, QA lead |
| Pilot migration | Workload move, controlled cutover, hypercare support | Migration lead, app owners, operations, clinical super users |
| Validation and adjustment | Workflow testing, incident review, optimization, go or pause decision | Clinical sponsors, QA, security, platform team |
| Scale-out rollout | Repeatable migration waves, governance checks, operational handoff | PMO, cloud team, support, department leaders |
Validate clinical outcomes, not just infrastructure
Teams often declare a wave successful because servers are up and response times look acceptable. That's not enough. Validation has to include end-to-end workflows used by clinicians, schedulers, billers, and support staff.
Focus test execution on:
-
Critical patient journeys such as admit, discharge, transfer, order entry, results review, and handoff workflows
-
Interface and data integrity checks across EHR, PACS, LIS, billing, and third-party platforms
-
Security and access validation for RBAC, MFA, break-glass access, and audit trail completeness
-
User acceptance with clinicians in realistic scenarios, not only scripted technical tests
Keep the legacy system longer than finance wants if it reduces clinical risk during validation. The overlap cost is often cheaper than a rushed cutover.
Formal stop/go checkpoints matter. Clinical leadership needs authority to pause a wave if workflow outcomes aren't holding. That governance discipline is what keeps a migration from becoming a technical exercise detached from care delivery.
Modernizing Operations with CI/CD and Observability
A migrated workload that still relies on manual changes, undocumented fixes, and fragmented monitoring hasn't really been modernized. It has just changed addresses. Day 2 operations are where the cloud starts paying off, or starts becoming expensive chaos.
The strongest operating model in healthcare pairs infrastructure as code, controlled deployment pipelines, and observability designed around service health and clinical workflows. That matters because migration failure patterns often begin with inconsistent post-cutover management. Manual adjustments in production create drift, drift breaks compliance evidence, and broken evidence turns every audit into a reconstruction project.
CI/CD has to be compliance-aware
Healthcare teams sometimes hear CI/CD and assume rapid-fire production releases. That's the wrong frame. In a regulated environment, CI/CD is mainly about making change repeatable, reviewable, and auditable.
A good pipeline should enforce:
-
IaC-only environment changes using tools such as Terraform, Pulumi, or CDK
-
Version-controlled approvals for infrastructure, application, and policy updates
-
Automated checks for configuration drift, secret handling, and deployment policy violations
-
Environment promotion rules so test, staging, and production don't diverge unpredictably
That approach aligns directly with modern custom software development practice. It reduces hand-built variation, which is one of the main causes of post-migration instability.
Observability should follow care workflows
Traditional monitoring tells you if a server is available. Observability tells you why a clinician couldn't complete an order or why an interface queue is growing. That's the difference between infrastructure awareness and operational insight.
A useful stack usually includes these layers:
| Layer | Purpose |
|---|---|
| Centralized logs | Correlate events across apps, interfaces, IAM, and cloud services |
| Metrics | Track latency, errors, queue depth, throughput, and resource pressure |
| Traces | Follow requests across APIs, services, and data pipelines |
| Alerting | Escalate by clinical impact, not only technical severity |
The key is to define service indicators around what hospital teams experience. Order latency. Results delivery delays. Authentication failures during shift change. Interface retries after a vendor timeout. Those signals help operations teams respond before clinicians start opening tickets.
Platform discipline creates room for innovation
Once pipelines and observability are stable, routine changes stop feeling dangerous. Teams can patch faster, onboard integrations with less friction, and evolve systems without rebuilding trust every release cycle.
That's a significant operational step change. Cloud migration becomes a platform capability, not a one-time project.
Unlocking AI-Driven Optimization and Managed Services
The most valuable outcome of healthcare cloud migration isn't infrastructure flexibility. It's what your organization can do once data, controls, and integration patterns are finally in usable shape. Predictive analytics, imaging workflows, automation, and operational decision support all become more realistic when data isn't trapped across brittle systems.
That opportunity comes with one legal and architectural trap that generic migration guides often miss. A critical but often-missed nuance is the gap between “HIPAA-eligible” and “HIPAA-compliant” services, as many advanced AI and machine learning services are not explicitly eligible, creating potential legal exposure for organizations, as explained in this healthcare cloud migration checklist. In plain terms, a cloud provider may offer powerful AI tooling, but your team still has to verify whether the exact service can be used for ePHI in your target design.

Build guardrails before AI use cases
The sequence matters. Don't start with the model. Start with the service boundary, data classification, retention rules, prompt handling, auditability, and human review requirements.
A practical AI readiness filter looks like this:
-
Use de-identified or limited datasets first where the use case allows it
-
Validate service eligibility before any protected data enters an AI workflow
-
Separate experimentation from production with clear controls and approval gates
-
Instrument every workflow so teams can trace data use, outputs, and operator actions
Cloud strategy becomes product strategy. A hospital or healthtech platform that has done migration properly can move from reactive reporting to more advanced use cases in a controlled way.
Use managed support where it removes operational drag
Many internal teams can architect the target state. Fewer can sustain cloud operations, security evidence, cost controls, release engineering, and AI enablement without overloading staff. That's where managed services become practical rather than optional.
The right external support model depends on what the hospital lacks most:
| Need | External support can cover |
|---|---|
| Platform operations | Monitoring, patching, incident response, environment hygiene |
| Engineering acceleration | Replatforming, APIs, pipelines, refactoring |
| AI enablement | Governance setup, model integration, workflow design |
| Product evolution | Turning internal tools into scalable platforms |
For organizations that need help spanning migration, modernization, and AI adoption, one route is combining AI development services, an AI implementation roadmap, and broader enterprise AI solutions. Bridge Global also offers custom healthcare software development and flexible software development service models for teams that need engineering capacity without building every specialty in-house.
The point isn’t to outsource responsibility. It’s to avoid burning out internal teams on platform maintenance when leadership expects them to deliver clinical and product innovation at the same time.
Frequently Asked Questions About Healthcare Cloud Migration
How long does a healthcare cloud migration usually take?
Most first-time hospital migrations take longer than leadership expects. Focused moves, such as VDI, archive storage, or a contained analytics workload, can often finish in 3 to 6 months. Larger programs that include core clinical systems, integrations, and operating model changes often run 18 to 36 months, a range that aligns with enterprise transformation timelines described by McKinsey on cloud transformations.
The schedule usually slips because of dependency mapping, interface remediation, security review, and validation in real clinical workflows. Provisioning cloud infrastructure is rarely the slow part.
Is lift-and-shift ever the right approach?
Yes, if the goal is clear.
I recommend lift-and-shift for workloads that are stable, poorly suited for immediate refactoring, or sitting on infrastructure with rising operational risk. It can buy time, reduce data center exposure, and create a cleaner starting point for later modernization.
The mistake is treating rehosting as the finish line. A HIPAA-eligible landing zone is only the beginning. If the target system still has brittle interfaces, weak auditability, or data structures that block downstream analytics and AI, the hospital has changed hosting, not capability.
Should hospitals choose single-cloud, hybrid, or multi-cloud?
The right model depends on constraints, not fashion.
Hybrid is common in healthcare because imaging, medical devices, latency-sensitive systems, and vendor hosting terms still tie parts of the estate to on-premises infrastructure. Multi-cloud can make sense for organizations with strict resilience requirements or teams that need specific platform services from different providers. Single-cloud is often the easiest option to govern well, which matters more than theoretical flexibility.
I usually advise hospital teams to decide based on identity design, network boundaries, logging, disaster recovery, and where protected health information is allowed to move. Architecture sprawl creates more risk than platform concentration in most first migrations.
What causes the most disruption during migration?
Undocumented dependencies cause more trouble than the cutover event itself.
Common failure points include incomplete interface inventories, inconsistent patient or provider identifiers, hard-coded IP allowlists, vendor appliances nobody wants to touch, and test plans that verify infrastructure but miss end-to-end clinical workflows. Downtime incidents often start months earlier, during assessment, when teams assume they understand how a legacy system behaves in production.
When should a hospital start planning for AI?
During the migration design phase, not after go-live.
Hospitals that wait usually find out too late that their migrated environment cannot support the AI use cases leadership wants to fund. The blockers are predictable. Missing metadata, weak data lineage, service boundaries that were never approved for PHI, and architectures that can host workloads in the cloud but cannot support governed model access, retrieval pipelines, or traceable outputs.
That is the gap generic migration guides miss. The best migration plan gets the workload off legacy infrastructure and prepares the data, controls, and platform services needed for future automation and AI.
If your team is preparing for its first major healthcare cloud migration, Bridge Global can support the work from strategy through implementation, with capabilities across compliant healthcare engineering, cloud modernization, data architecture, integrations, and AI-enabled product development.
About Preethi Saro Philip
Preethi Saro Philip is a Post Graduate Research Degree holder in Economics with more than 10 years of experience in writing, editing, research and teaching. She has an intense passion for content crafting and calls herself a ‘wordsmith’. She enjoys writing on wide-ranging topics including business, technology, health & lifestyle, education, environment etc.
View all posts by Preethi Saro Philip →