


Cloud Infrastructure for Healthcare Systems: A Guide for You
Cloud strategy in healthcare stopped being a side conversation once it became infrastructure. The global healthcare cloud infrastructure market was estimated at USD 76.72 billion in 2024 and is projected to grow at a 16.66% CAGR from 2025 to 2030, according to Grand View Research's healthcare cloud infrastructure market analysis. That scale changes the question from “Should we use cloud?” to “Which workloads belong where, under what controls, and for what future state?”
For CTOs, that decision sits at the intersection of architecture, compliance, operating cost, interoperability, and AI readiness. Cloud infrastructure for healthcare systems isn't just about moving servers. It determines how reliably clinicians access records, how quickly product teams ship integrations, how safely PHI moves through analytics pipelines, and whether your data platform can support machine learning without forcing a second transformation later.
Why Cloud Is Non-Negotiable for Modern Healthcare
Healthcare organizations are under pressure from every direction at once. Clinical systems need to stay available. Patient and member experiences need to improve. Product teams need to ship faster. Security and privacy teams need tighter control, not looser control. Cloud is the only practical environment that can support all of those needs at enterprise scale without locking every improvement behind long hardware cycles.
That's why cloud infrastructure for healthcare systems has become a board-level issue rather than a hosting decision. The market's size and projected growth show that cloud now sits in the same category as core healthcare infrastructure, not optional innovation. It's where health systems, payers, and digital health platforms increasingly run EHR-adjacent services, imaging workflows, analytics stacks, and remote care applications.
A mature cloud posture also changes how technical leaders sequence modernization. Instead of treating compliance, interoperability, and AI as separate programs, strong teams treat them as connected design outcomes. Identity architecture affects auditability. Data platform choices affect model training later. Integration strategy affects migration cost.
Practical rule: If your cloud program can't explain how data moves, who can access it, how it's monitored, and how it will support future analytics, you don't have a cloud strategy. You have hosting with extra complexity.
The organizations that move well usually avoid one common mistake. They don't start with vendor preference. They start with workload classification, regulatory boundaries, integration realities, and operating model. That's especially important when you're planning custom healthcare software development around clinical workflows, patient-facing products, or regulated data services.
Choosing Your Blueprint Cloud Architecture Patterns
Architecture decisions in healthcare age slowly. Once data pipelines, identity boundaries, integrations, and vendor-specific services are in place, changing direction gets expensive. A weak blueprint creates friction for years. A good one keeps options open without introducing unnecessary complexity.
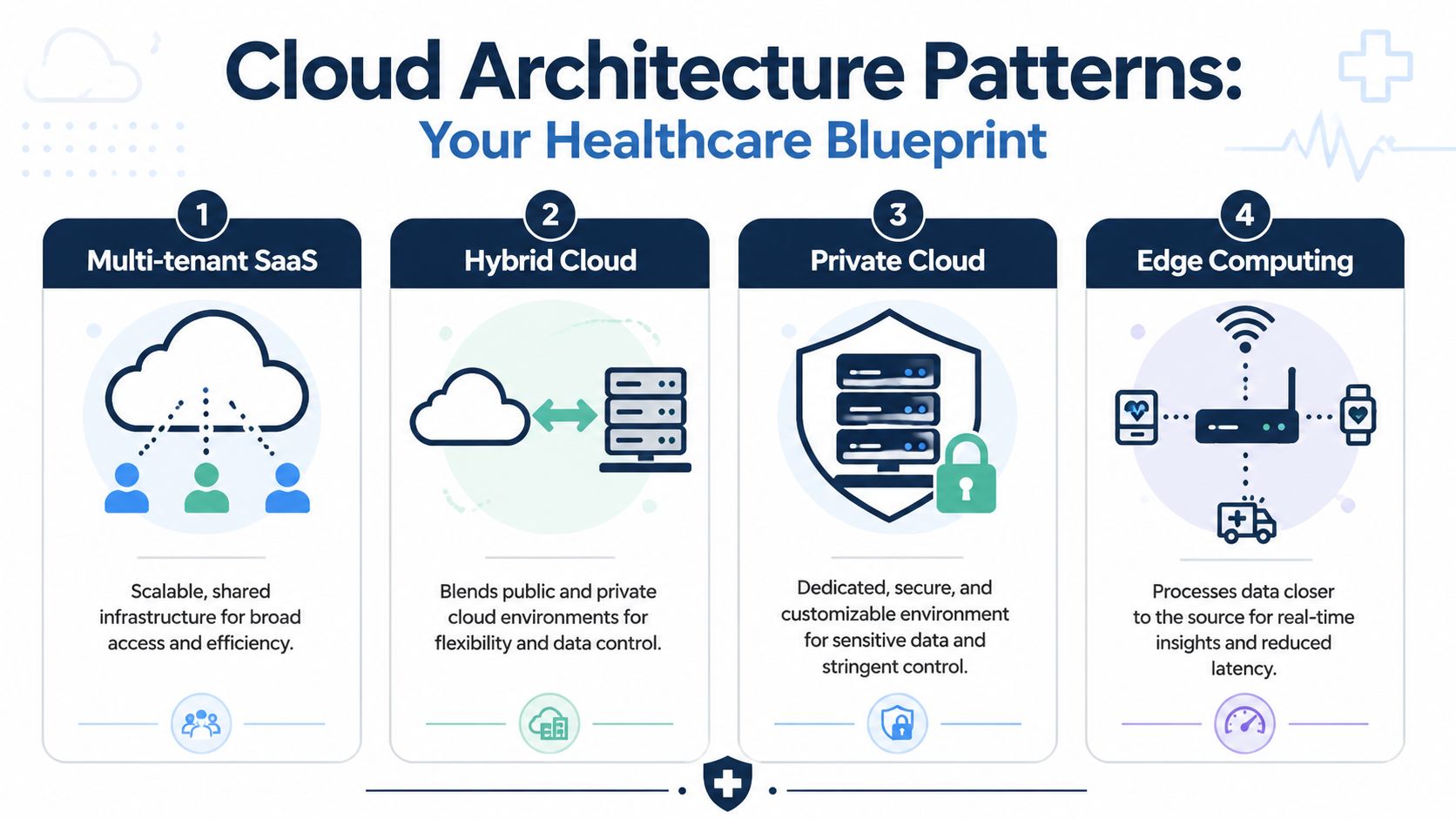
Four patterns that matter in healthcare
Multi-tenant SaaS works best when you're building a repeatable product for many customers with largely similar workflows. Think patient engagement platforms, scheduling products, care coordination tools, or payer-facing workflow systems. The operating advantage is obvious. You standardize deployment, patching, observability, and release management across customers. The trade-off is control. Tenant isolation, data partitioning, and customer-specific configuration become engineering concerns from day one.
Hybrid cloud fits organizations that can't move everything at once, which is most of healthcare. A hospital may keep part of an imaging archive, a legacy EHR integration engine, or device-connected workflow on-premises while shifting analytics, portals, data exchange layers, and automation services to the cloud. Hybrid is often the most realistic pattern. It's also where teams underestimate complexity. Latency, network dependencies, identity federation, and operational handoffs create failure points unless they're designed explicitly.
Private cloud still matters for organizations that need tighter environmental control or have workloads with strict governance requirements, specialized hardware dependencies, or limited tolerance for multi-tenant abstractions. Private environments can support stronger customization and policy alignment, but they also shift more operational burden back to the organization or managed service partner.
Edge computing belongs near the source of care when decisions can't wait for round-trip trips to a central cloud region. Connected medical devices, bedside applications, local imaging workflows, and environment-sensitive monitoring often benefit from processing closer to where the data is produced. Edge reduces latency and can improve resilience, but only if teams have a clear synchronization and recovery strategy.
Healthcare cloud architecture models compared
| Model | Best For | Key Benefit | Main Challenge |
|---|---|---|---|
| Multi-tenant SaaS | Product companies serving many healthcare customers | Standardized scaling and operational efficiency | Tenant isolation, customization boundaries |
| Hybrid cloud | Providers with legacy systems and gradual migration plans | Balances modernization with operational continuity | Integration complexity and cross-environment dependencies |
| Private cloud | High-control environments with specialized governance needs | Dedicated control and deeper customization | Higher operational overhead |
| Edge computing | Real-time care workflows and device-adjacent processing | Lower latency and local resilience | Data synchronization and distributed operations |
What usually works and what usually fails
The architecture pattern matters less than the discipline behind it. A recent review notes that healthcare cloud adoption still faces high execution and maintenance costs, fragmented data integration, and multi-cloud interdependency risks, while also warning that provider changes can make personal data less secure, as discussed in this review of cloud adoption challenges in healthcare. That’s why “we’ll use hybrid” or “we’ll go multi-cloud for resilience” isn’t a strategy by itself.
What works is boring in the right way:
-
Clear workload placement: Decide which systems must stay close to legacy dependencies and which can move into managed services.
-
Explicit integration ownership: Name the team responsible for APIs, event flows, message transformations, and rollback behavior.
-
Exit-aware design: Keep data export, schema portability, and service substitutions visible before platform-specific features spread everywhere.
Hybrid and multi-cloud can reduce concentration risk. They can also multiply operational risk if the team doesn’t standardize identity, observability, and integration contracts.
Fortifying Your Foundation Compliance and Security by Design
Most healthcare cloud failures don’t begin with a dramatic breach. They begin with design shortcuts. An over-permissioned service account. A backup policy that no one tested. A migration path that ignores throughput limits. A production workload that exhausts resources under normal clinical demand.
Shared responsibility is real, but it’s not enough
Cloud providers secure the underlying platform. Your organization still owns configuration, identity, data handling, application logic, logging, key usage, and operational response. In healthcare, that means compliance and security have to be designed together. You can’t separate the “policy part” from the “engineering part” and expect the system to hold.
Teams planning HIPAA-aligned or HITRUST-oriented environments should treat security controls as architecture components, not later-stage hardening tasks. If identity boundaries, encryption flows, and audit trails aren’t built into the platform, compliance work turns into paperwork layered over fragile systems.
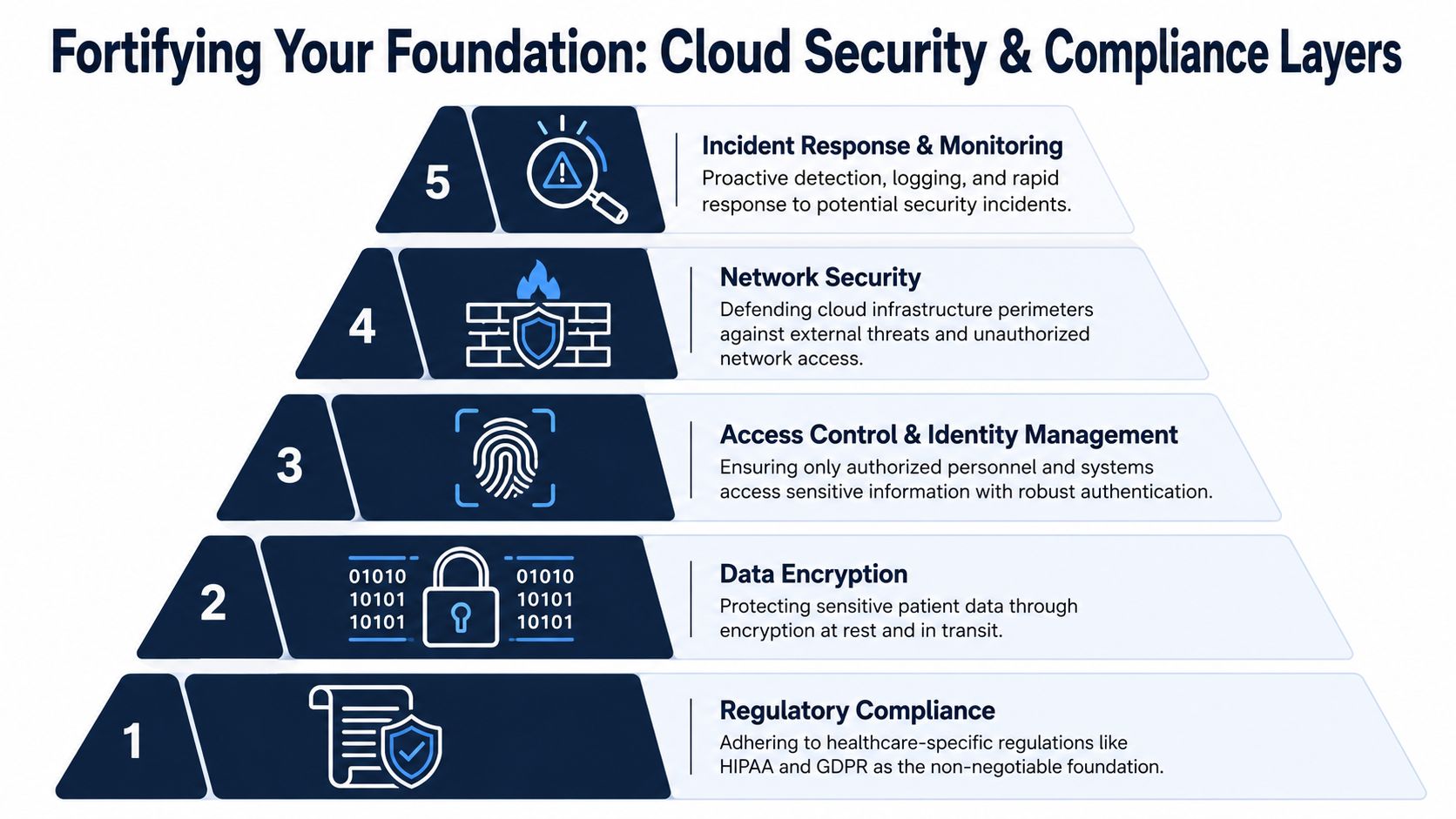
The controls that deserve engineering attention first
The most important controls aren’t glamorous:
-
Least-privilege IAM: Every human and service identity should have only the permissions required for its role. Break-glass access should be documented, monitored, and temporary.
-
Encryption design: Encrypt PHI at rest and in transit. For sensitive workloads, define how keys are created, rotated, scoped, and audited. Managed keys can be enough for many systems. Some workloads justify tighter key custody through managed HSM patterns.
-
Continuous compliance checks: Don’t rely on one-time audits. Use policy-as-code, configuration baselines, and drift detection so misconfigurations are caught before they become incidents.
-
Backup and disaster recovery testing: Backups don’t count until restore procedures are tested under realistic conditions, including access failures and regional disruption.
-
Network segmentation: Isolate workloads by trust zone, application role, and data sensitivity. Flat networks create an avoidable blast radius.
A practical summary from healthcare cloud migration research is that the main engineering failure modes are not just security-related. They include resource exhaustion, unpredictable performance, data-transfer bottlenecks, and data lock-in, according to this study on cloud adoption and migration issues in healthcare. That finding aligns with what architecture teams see in the field. Availability issues often come from capacity assumptions and data movement patterns, not only attacker behavior.
Security operations have to match clinical reality
Healthcare systems don’t operate on neat business-hours assumptions. Access patterns spike. Devices reconnect unpredictably. Clinical users need speed under pressure. Good security design accounts for that reality without relaxing control.
For internal planning, many CTOs also compare external operational guidance on how IT teams can resolve medical office IT challenges because smaller practice environments often expose the same root issues seen at a larger scale: inconsistent device management, weak access discipline, and fragmented support ownership.
A strong implementation usually includes dedicated cybersecurity services capability for threat modeling, log design, access review, and incident response planning. That doesn’t replace internal ownership. It fills the gaps between infrastructure deployment and operational readiness.
Security by design means every critical workload can answer four questions at any time: who accessed it, what changed, where the data moved, and how recovery works.
Breaking Down Silos: Interoperability and Modernization
Cloud becomes most valuable in healthcare when it stops being a hosting layer and becomes an integration layer. That’s where long-standing data silos start to break. EHR modules, payer systems, labs, imaging platforms, devices, patient apps, and analytics environments don’t need to be rewritten into one giant system. They need reliable ways to exchange data, events, and identity context.
Why cloud-native interoperability changes the equation
FHIR-based APIs, event-driven integration, managed messaging, API gateways, and secure identity federation make healthcare interoperability more practical than it was in earlier on-premise stacks. The cloud doesn’t solve semantic mismatch by itself, but it gives teams better tooling to standardize authentication, expose services, log transactions, and enforce policy.
That matters because most modernization efforts fail when they treat integration as a side task. It isn’t. In healthcare, integration is the system. If orders, observations, imaging metadata, claims status, consent state, or patient-generated data can’t move predictably, the user-facing application will feel broken no matter how polished the UI looks.
The fastest route to modernization is rarely a full replacement. It’s usually a controlled extraction of the most valuable workflows into APIs, services, and event contracts.
The migration decision isn’t lift-and-shift versus rebuild
Legacy systems deserve different treatment depending on their risk, value, and constraints. The classic migration patterns still apply, but healthcare teams need a stricter lens:
-
Rehost when the application is stable, tightly coupled, and not worth rewriting yet.
-
Replatform when you can improve operations through managed databases, container hosting, or automated deployment without changing core business logic.
-
Refactor when the current design blocks interoperability, analytics, or security goals.
-
Retire when the system survives only because no one wants to own the replacement decision.
-
Retain when a system must stay where it is because of vendor limitations, device dependencies, or regulatory posture.
-
Replace when a commercial or newly built platform removes more complexity than it adds.
The mistake is using one migration pattern for every application. A PACS-adjacent archive, a scheduling portal, and an internal care management tool shouldn’t all follow the same path.
What a practical modernization program looks like
A credible program usually starts with a dependency map, not a target-state slide deck. Teams inventory interfaces, data stores, identity touchpoints, and operational runbooks. Then they classify systems by clinical criticality and modernization effort.
That’s where deep healthcare integrations’ expertise matters. It often sits next to custom software development because the hard part isn’t only connecting systems. It’s designing the custom workflow layer that makes those integrations usable, observable, and maintainable.
The Economics of Care Cloud Cost and Performance Optimization
Cloud economics in healthcare get distorted when teams look only at infrastructure line items. The complete cost picture includes data movement, storage tiering, environment sprawl, idle compute, duplicated integration logic, on-call burden, and the operational drag of poor performance. If you miss those factors, your cloud bill becomes a symptom, not the problem.
Where healthcare cloud spend actually accumulates
Imaging, analytics, archival retention, remote access, and batch-heavy integration workloads create unusual cost pressure. DICOM repositories are large. Clinical data pipelines are noisy. Development teams spin up environments quickly. Interface engines and ETL jobs move more data than many leaders realize. Then, AI pilots begin consuming copies of the same datasets in parallel workspaces.
A healthy cloud program brings engineering and finance together through FinOps. That doesn’t mean finance approves every resource. It means product, engineering, architecture, and finance share visibility into unit cost, environment hygiene, data lifecycle rules, and forecast assumptions.
Performance tuning can’t be separated from cost control
Cheap systems that clinicians can’t rely on aren’t cheap. Latency in telehealth, document retrieval, prior authorization workflows, or patient portal traffic creates downstream cost through user friction and operational workarounds. The better strategy is to optimize cost and performance together.
Healthcare IT leaders report concrete operational value here. 63% cited reliability and recovery as the biggest advantage of cloud, and 56% cited better accessibility for remote users, according to NetSuite’s overview of healthcare cloud adoption and benefits. Those are practical outcomes, not abstract architecture goals.
Cost controls that usually hold up over time
Some cost practices create one-time savings. Others become operating discipline:
-
Right-size by workload pattern: Clinical APIs, analytics jobs, and background ingestion pipelines have different usage curves. Treat them differently.
-
Use storage lifecycle rules: Not every dataset needs premium access forever.
-
Tag aggressively: If a team can’t attribute spend to product, environment, or business owner, governance will decay.
-
Consolidate duplicated pipelines: Rebuilding the same transform logic across departments creates an invisible expense.
-
Review data egress assumptions early: Cross-region, hybrid, and partner-heavy architectures can generate unnecessary transfer costs.
-
Set performance SLOs before optimization: Otherwise, teams tune the wrong thing.
For leaders building stronger operating discipline, this guide to effective cloud cost controls is a useful external reference because it frames optimization as an ongoing management practice rather than a one-time cleanup.
The Future of Health: Unlocking AI and ML with Cloud Native Tools
Most healthcare AI programs fail before the model does. They fail in data access, environment provisioning, governance, feature preparation, and deployment friction. That’s why cloud readiness matters so much. If your infrastructure can’t support governed data pipelines, reproducible environments, and controlled model serving, AI remains a slide deck.

What cloud-native AI makes practical
In healthcare, cloud-native AI usually starts with narrow, high-value tasks. Natural language processing can structure clinical notes, intake text, and prior authorization narratives. Computer vision can support image workflow triage and quality review. Predictive models can help forecast demand, identify care gaps, or flag operational anomalies.
The enabling pattern is consistent. Data lands in governed storage. Pipelines clean and label it. Managed services such as AWS SageMaker, Google Vertex AI, and Azure Machine Learning provide training, experiment tracking, deployment options, and model operations scaffolding. Serverless functions, event buses, and containerized APIs handle inference workflows around the model.
Future-ready teams design the AI path early
AI amplifies every architectural choice made earlier. If patient identity is fragmented, features become unreliable. If audit logs are incomplete, model governance gets weak. If integration contracts vary by customer or facility, deployment becomes expensive.
That’s why the best AI strategy in healthcare often starts as an infrastructure strategy. Teams define data domains, access policies, annotation workflows, model-serving boundaries, and human review loops before they scale experimentation.
A useful reference point is this whitepaper on AI hospital automation in healthcare operations, which focuses on where cloud-backed automation can support operational processes rather than treating AI as a standalone initiative.
AI readiness in healthcare isn’t about buying a model platform first. It’s about making data, controls, and deployment pathways dependable enough that models can survive contact with clinical operations.
For organizations moving from platform work into execution, common next steps include defining an AI implementation roadmap, evaluating AI development services, and deciding where enterprise AI solutions fit into the broader product and data strategy.
Building Your Team: Selecting the Right Vendor and Partner
Cloud vendor selection in healthcare gets oversimplified fast. Teams compare feature lists, pricing calculators, and service catalogs, then assume the hard part is done. It isn’t. The key decision is whether the platform and the delivery partner can support your regulatory posture, integration complexity, and operating model for years.
How to evaluate a cloud platform for healthcare workloads
Start with workload fit, not brand preference. Ask which services are appropriate for PHI-adjacent and PHI-bearing workflows, how identity integrates with your existing directory and access policies, what data residency options exist, and how well the platform supports interoperability patterns you already need.
Also, look at boring operational details:
-
Healthcare service maturity: Can the platform support common patterns around APIs, logging, key management, backups, analytics, and event workflows without heavy custom engineering?
-
Governance tooling: Does it help your team enforce policy consistently across accounts, subscriptions, or projects?
-
Partner ecosystem: Can your implementation team find healthcare-aware support for integrations, data engineering, and compliance work?
-
Portability trade-offs: Which managed services save time now, and which ones could increase future migration effort?
The implementation partner matters as much as the platform
A technically competent partner can still struggle if they don’t understand healthcare workflows. Clinical operations, payer processes, consent handling, identity matching, device integrations, and audit expectations affect architecture choices every week during delivery.
A practical partner review usually includes these checks:
-
Ask for relevant delivery evidence. Review client cases that show regulated platforms, integration-heavy systems, or healthcare-adjacent products.
-
Understand team structure early. Compare available software development service models so you know who owns architecture, delivery management, QA, DevOps, and support.
-
Test product thinking, not just coding. If you’re building a platform business, ask about SaaS product development, tenant isolation, release governance, and operational scaling.
-
Verify healthcare-specific judgment. A good partner should discuss FHIR, data partitioning, auditability, resilience, and migration trade-offs without needing to be prompted.
One practical option in this space is working with a healthtech software development partner that combines healthcare engineering, cloud enablement, and AI-oriented product work. The key is not the label. It’s whether the team can translate strategy into a delivery model that holds up under compliance review and production load.
Questions worth asking before you sign
Use direct questions. How do you handle PHI in lower environments? How do you enforce least privilege across delivery teams? How do you test restores? Who owns interface validation? What’s your rollback approach during release windows that affect clinical users?
If a partner answers with only process language and no concrete engineering patterns, keep looking.
Frequently Asked Questions About Healthcare Cloud
Is public cloud appropriate for regulated healthcare workloads?
Yes, if the workload is designed correctly. The issue usually isn’t “public cloud versus private cloud” in isolation. The issue is whether identity, encryption, logging, access review, backup recovery, and data handling are engineered to match the workload’s sensitivity and operational reality. Many teams use a mix of public cloud, private environments, and retained on-premise systems because different workloads have different constraints.
Should a hospital choose hybrid by default?
Not by default, but often by necessity. Hybrid makes sense when legacy EHR, imaging, device, or facility-specific dependencies can’t move cleanly. It becomes a bad default when teams use it to postpone architecture decisions. If you choose hybrid, define integration ownership, observability, identity boundaries, and a target operating model early.
Is multi-cloud worth it for resilience?
Sometimes. Multi-cloud can reduce dependency on one provider, but it can also increase complexity in identity, networking, monitoring, policy enforcement, and data movement. It’s worth it when there’s a clear business or resilience case, and the team can operate it well. It’s not worth it as a slogan.
What should move to the cloud first?
Start with workloads that produce operational value without creating avoidable clinical risk. Good candidates are integration layers, patient-facing applications, analytics platforms, reporting services, and selected internal tools with manageable dependencies. Systems with tight coupling to devices, brittle vendor interfaces, or unclear data boundaries usually need more preparation.
How should CTOs think about AI readiness?
Treat AI readiness as a data and platform capability, not a tooling purchase. You need governed data access, traceable pipelines, clear model-serving boundaries, and operational review processes. If those aren’t in place, managed ML platforms won’t solve the core problem.
What usually derails cloud migrations in healthcare?
Poor dependency mapping, weak access controls, underplanned data movement, and unrealistic assumptions about legacy behavior. Another common issue is splitting responsibility too loosely between infrastructure, application, security, and integration teams. In healthcare, those boundaries have to be tightly coordinated because a failure in one layer usually shows up as a care delivery issue somewhere else.
When does refactoring make more sense than rehosting?
Refactor when the current application blocks interoperability, cost control, resilience, or future product direction. Rehost when the application is stable, and the main objective is relocation with minimal change. The right answer depends on business value, technical debt, and how central that system is to your long-term platform.
Healthcare cloud decisions are easier when architecture, compliance, integration, and AI planning are handled as one program instead of separate initiatives. If you’re evaluating your next move, Bridge Global can be considered as one implementation partner for secure platform design, modernization planning, and healthcare product engineering.
About Preethi Saro Philip
Preethi Saro Philip is a Post Graduate Research Degree holder in Economics with more than 10 years of experience in writing, editing, research and teaching. She has an intense passion for content crafting and calls herself a ‘wordsmith’. She enjoys writing on wide-ranging topics including business, technology, health & lifestyle, education, environment etc.
View all posts by Preethi Saro Philip →