


Healthcare Automation Architecture for Scalable Solutions
Healthcare automation now fails or succeeds at the architecture level. The teams that get real value from automation are the ones that treat it as a systems design problem early, before workflows, models, and integrations start to compete with compliance requirements.
In production, weak results usually trace back to architecture decisions made too late. A team adds automation on top of legacy workflows, postpones audit design, and assumes exceptions can be handled manually. That approach breaks fast in healthcare. Prior authorization cases branch. EHR data arrives incomplete. Human review, consent rules, and retention requirements shape the workflow as much as the business logic does.
A healthcare automation system that holds up under real operating conditions needs multiple layers with clear responsibilities. It needs event handling, strong integration boundaries, policy enforcement, and a migration plan that accepts the reality of existing EHRs, billing platforms, device feeds, and analytics environments.
That is the standard I use when designing automation platforms for provider, payer, and digital health products. The goal is not architectural purity. The goal is a system that can orchestrate work across clinical and operational processes, preserve traceability, support AI where it adds value, and stay compliant when the process leaves the happy path.
The sections that follow focus on how to build that system. They cover the architectural patterns that work in production, the layers that should be separated from day one, the governance controls that cannot be deferred, and the implementation choices that help CTOs and product leaders move from pilot automations to a platform. If you are planning a broader transformation effort, these decisions also align with an AI implementation roadmap.
Why Healthcare Automation Architecture Matters Now
Analysts and product teams can point to strong demand for healthcare automation. The harder question is what separates an automation program that survives production from one that stalls after a few pilots. In practice, the answer is architecture.
The timing matters because the underlying environment has changed. A typical healthtech workflow no longer lives inside one application and one data model. It spans EHR APIs, payer transactions, document pipelines, messaging queues, identity services, analytics stores, and, in many cases, AI services that introduce their own approval, monitoring, and traceability requirements. Each new integration adds value, but it also adds state to manage, failure modes to contain, and compliance boundaries to enforce.
That is why architecture has moved from a technical concern to an operating constraint.
Operational pressure now shows up at the integration boundary
The biggest failures I see are not caused by the core workflow logic. They happen at the edges. An eligibility response arrives late. A prior authorization payload is missing an attachment. A consent flag in one system does not match the status stored in another. Staff can often recover from one of these issues manually. They cannot recover from hundreds of them per day without cost, delay, and audit risk.
Healthcare organizations are trying to automate across systems that were never designed to behave like one platform. That creates a specific set of design requirements:
Reliable cross-system coordination: The system needs clear contracts between EHRs, billing platforms, CRM tools, and third-party services, so one schema change does not break an entire workflow.
Asynchronous processing by default: Timeouts, retries, duplicate messages, and delayed callbacks are normal conditions, not edge cases.
Human review with context: Clinical and operational exceptions need routing, case history, and decision trails, not a generic error queue.
A production architecture has to treat those conditions as baseline reality.
Safe automation depends on architectural separation
A workflow can look excellent in a demo and still fail in production within weeks. Clean sample data hides most of the hard parts. Real environments have partial records, conflicting updates, policy changes, and downstream systems with different uptime and throughput limits.
That is why I push teams to evaluate automation readiness in architectural terms. Can the platform track workflow state independently of source systems? Can it enforce policy decisions consistently across channels? Can it preserve an audit trail without forcing every service team to build its own logging model? Can it introduce AI into one step without making the whole process harder to validate?
If the answer is no, scaling automation usually increases operational drag instead of reducing it.
The real decision is about control
Healthcare leaders rarely struggle to find candidate use cases. They struggle to build enough control into the platform to automate them safely. The architecture has to support change without forcing full-system retesting every time a payer rule, intake form, integration mapping, or review path changes.
That is the reason this matters now. The pressure is no longer just to automate a task. It is to build a system that can absorb more workflows, more integrations, and stricter oversight without becoming slower, riskier, or harder to operate.
Foundational Architectural Patterns for Healthtech
A 2024 systematic review of 89 studies found that healthcare architecture work heavily favors microservices and event-driven patterns, especially in systems that need to support standards such as HL7 FHIR and real-time operations (systematic review of healthcare architectural patterns). That trend makes sense in production. Healthcare automation rarely fails because teams picked the wrong framework. It fails because the architecture cannot isolate change, absorb integration volatility, or keep workflow state visible under regulatory scrutiny.
Legacy platforms were usually built as one application with one deployment path, one database boundary, and one release train. That approach can still work for a tightly scoped product. It breaks down once prior authorization, intake, patient communications, billing, and audit requirements start changing at different speeds.
Modern healthtech systems work better when they are designed around bounded domains. Identity and access, intake, clinical workflow, payer orchestration, notification delivery, and audit logging should not all live in the same code path. They should communicate through versioned APIs and events, with clear ownership and failure handling rules.
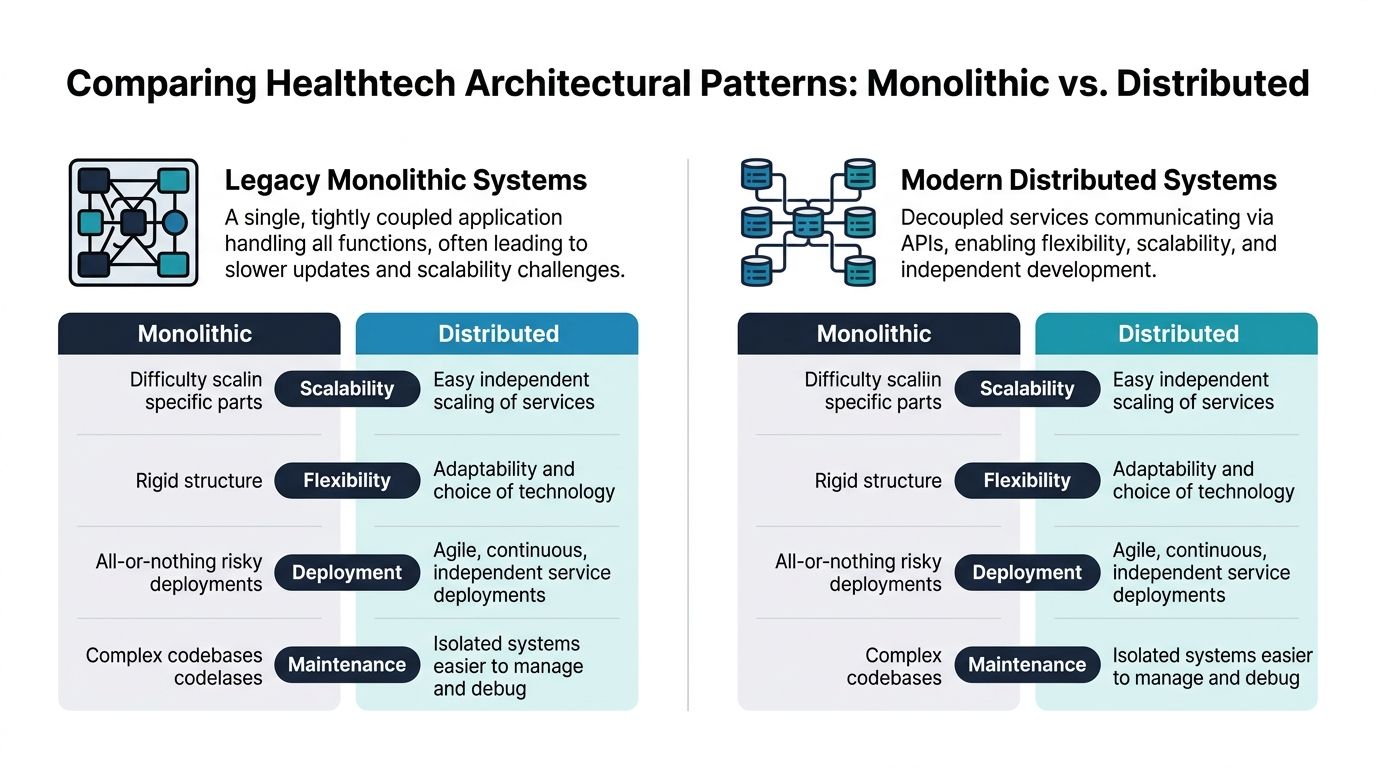
Why monoliths break down
Monoliths are still useful. For an MVP, a narrow internal tool, or a product with one core workflow, they reduce coordination overhead and can be easier to validate early.
The problem appears later. A payer rule update should not force full regression testing across scheduling, clinical documentation, and patient messaging. In many health systems, that coupling is exactly what slows releases, increases validation cost, and turns small changes into cross-team incidents.
| Pattern | Works well for | Breaks when |
|---|---|---|
| Monolith | Early-stage products, limited workflows, small teams | Release cycles slow, integrations grow, and one defect affects multiple functions |
| Microservices | Clear domain ownership, independent releases, complex integrations | Teams lack service boundaries, observability, or API discipline |
| Event-driven architecture | Real-time triggers, asynchronous workflows, state tracking | Event contracts are weak or idempotency is missing |
Why microservices and events fit healthcare better
Microservices fit healthcare because the business domains are already separate. Consent management changes under a different set of rules than coding. Scheduling has different uptime and latency needs than claims adjudication. A service boundary gives each area its own release cycle, test scope, and operational profile.
Event-driven design solves a different problem. Healthcare workflows do not progress in a neat sequence. Eligibility responses arrive late. Lab systems send updates out of order. Human review inserts pauses that no synchronous request chain handles well. Events let the system record state transitions as they happen and resume work when the next signal arrives.
Used together, these patterns give teams practical control. Services own decisions inside their domain. Events coordinate long-running processes across domains. That combination is usually more maintainable than a large synchronous API graph.
What teams get wrong with distributed systems
Distributed systems add failure modes. I see the same mistakes repeatedly in platform reviews and recovery projects.
Shared database shortcuts: Teams split the application into services but keep one database schema. The coupling remains, and schema changes become harder to coordinate.
Too many synchronous dependencies: One request fans out across several services, each with its own timeout and retry behavior. Latency rises, outages spread, and the system starts acting like a distributed monolith.
Weak event contracts: If payloads are loosely defined, downstream consumers end up parsing unstable fields and building service-specific exceptions.
No idempotency strategy: In healthcare, duplicate messages are normal. Without idempotent consumers and replay-safe handlers, retries create duplicate tasks, records, or notifications.
Thin observability: Logs alone are not enough. Teams need tracing, correlation IDs, queue visibility, and service-level alerts tied to workflow outcomes.
A distributed architecture only works when ownership and contracts are explicit. Each service needs a clear bounded context. Each event needs a schema, versioning rules, and retry behavior. Each critical workflow needs an authoritative state store so operators can see what happened, what is waiting, and what needs intervention.
For CTOs and product leaders, the design test is practical. Can one team change authorization logic without redeploying patient intake? Can delayed payer responses be replayed safely? Can auditors trace who triggered a decision, which rule executed, and which downstream systems were updated? If the answer is no, the architecture is not ready for regulated automation at scale.
If you are evaluating a healthtech software development partner or reviewing your internal platform strategy, use that standard. The architecture has to isolate change, tolerate partial failure, and keep operational evidence intact across every regulated workflow.
The Five Essential Layers of a Modern System
Most architecture diagrams fail because they mix everything together. Data pipelines, user workflows, model hosting, compliance controls, and infrastructure all end up in one picture. That's not useful for delivery. Teams need clear separation of concerns.
A production-grade healthcare automation platform needs five interoperable layers: infrastructure, data, algorithm, application, and security/compliance. That structure keeps models accountable throughout their lifecycle and gives each team a clear operating boundary (five-layer healthcare automation architecture).
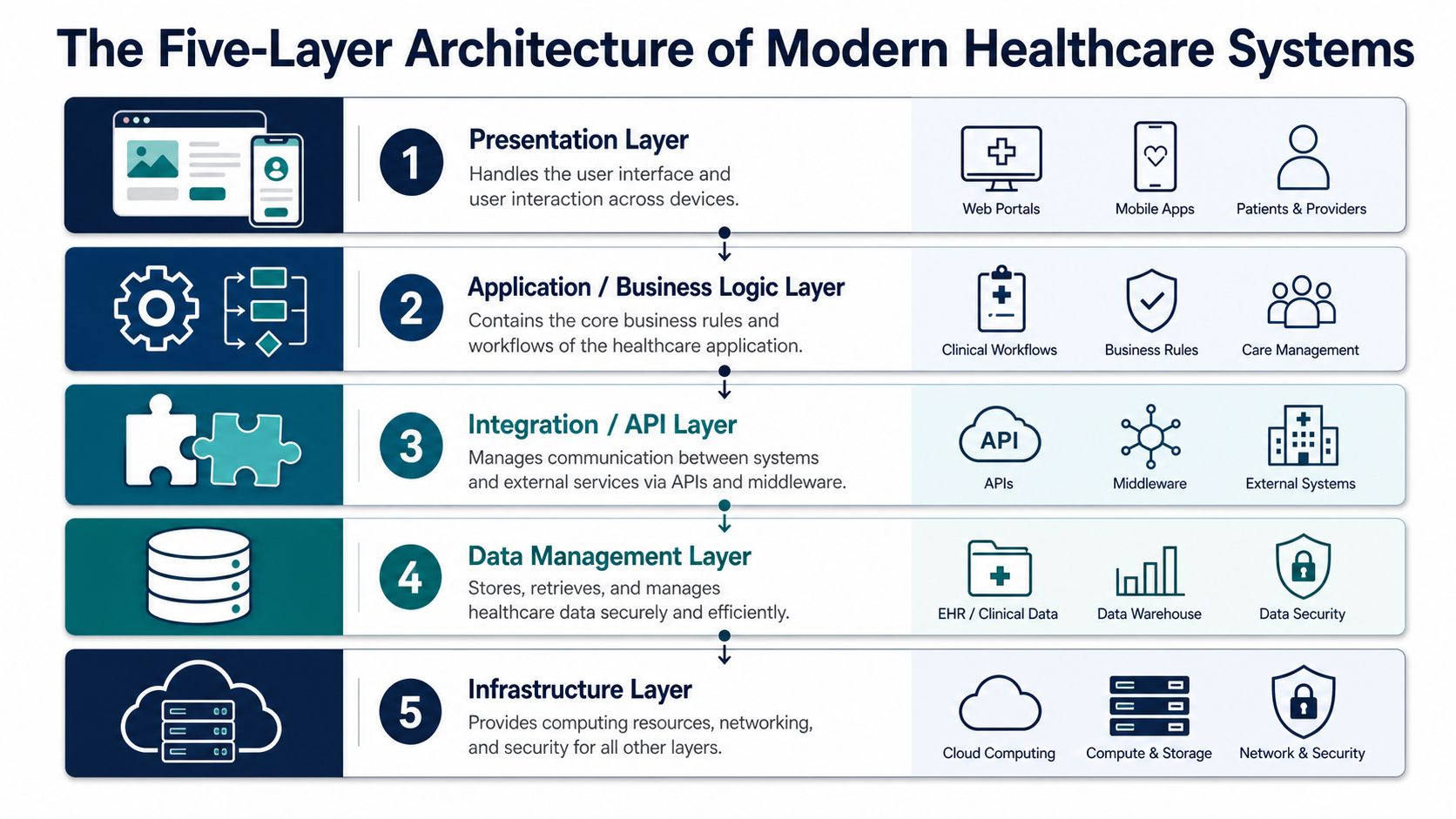
Infrastructure and data
The infrastructure layer is where compute, storage, networking, and deployment foundations live. In real systems, this includes your cloud environment, Kubernetes clusters or container services, managed databases, secrets handling, key management, observability stack, and backup strategy. This layer should be boring. If it's unstable, nothing above it matters.
The data layer standardizes how information enters and moves through the system. In healthcare, this usually means supporting HL7 FHIR for interoperable resources, while still handling older HL7v2 feeds, flat files, device output, and imaging standards where needed. Data normalization belongs here, not scattered inside business services.
A practical data layer usually includes:
Ingress adapters: FHIR APIs, batch importers, EHR connectors, and device listeners
Canonical models: Internal representations for patients, encounters, orders, and workflow events
Validation services: Schema checks, terminology mapping, and quality rules
Storage zones: Transactional stores for live workflows and analytical stores for reporting or model features
Algorithm and application
The algorithm layer is where AI and rule-based decisioning belong. This includes model training pipelines, validation workflows, model registry controls, prompt and policy templates where relevant, and the serving endpoints that expose predictions or draft outputs. Don't bury model logic in the application layer. That makes validation and version control harder.
The application layer orchestrates workflows that users and downstream systems depend on. Intake automation, authorization routing, coding support, claims workflows, exception queues, and review dashboards sit here. This layer should call lower layers through stable interfaces rather than reaching directly into raw source systems.
Design checkpoint: If a workflow engine has direct custom logic for every integration, your application layer is already taking on integration debt.
Security and compliance
The security and compliance layer cuts across everything, but it still needs explicit architecture. It covers identity, access control, encryption policy, audit logging, privacy handling, retention controls, and governance workflows for change approvals. In healthcare, teams that treat this as a final review phase usually end up redesigning core pathways later.
A strong healthcare automation architecture also benefits from one additional mental model. Keep an operations plane separate from business workflows. Monitoring, alerting, service health, audit review, and incident response shouldn't compete with front-line workflow execution.
For teams building regulated platforms through custom healthcare software development and deep healthcare integrations, this layered approach is what turns a collection of tools into a maintainable system.
Data Flow Governance and Integration
Healthcare automation fails subtly when data contracts are weak. The workflow may look complete in a demo, but the production path starts to drift the moment one EHR sends a field in a different structure, a payer changes its response pattern, or a device stream arrives out of sequence. Integration design is really data governance design under load.
The first rule is simple. Don't let source systems define your operating model. EHRs, billing systems, PACS environments, device feeds, and partner APIs all speak differently. If each downstream workflow consumes source-native payloads directly, every workflow becomes fragile.
Build a governed data movement model
Use an ingestion layer that accepts multiple formats and maps them into canonical domain objects. For example, patient identity, coverage, encounter state, order status, and task events should have clear internal representations even if upstream systems differ. That lets the rest of the platform reason about healthcare operations consistently.
A practical flow usually looks like this:
Ingest the source event through FHIR API calls, interface engines, file drops, or partner APIs.
Normalize and validate against canonical schemas and terminology expectations.
Enrich the event with reference data, consent status, or workflow context.
Publish to orchestration so workflow engines and downstream services react consistently.
Persist lineage and audit state so every decision can be traced.
Where teams usually introduce risk
The most common integration mistake is pushing transformation logic outward into many services. One team maps insurance coverage in the intake service. Another remaps it in prior auth. A third remaps it in claims support. Eventually nobody knows which interpretation is authoritative.
The better pattern is central stewardship for shared semantics, then local business logic for workflow-specific actions.
Keep source adapters thin: They should translate and authenticate, not own business rules.
Separate event transport from business meaning: A message queue moves the event. Domain services decide what it means.
Track lineage from ingest to action: You need to know which source record informed which automated step.
Version your schemas: Healthcare integrations break when change happens without notice.
Clean data flow isn't just an engineering concern. It's what makes automated decisions explainable to operations teams and auditors.
For a deeper treatment of policies, stewardship, and lifecycle controls, as we explored in our guide to healthcare data governance, governance works only when it's embedded in the architecture rather than documented beside it.
FHIR matters, but it isn't the whole story
FHIR is the right backbone for many modern workflows, but it won't remove all integration complexity. Real environments still contain legacy interfaces, proprietary exports, image systems, and operational tools that don't behave like clean FHIR-native platforms. Good architecture accepts that reality.
That's why the integration bus, event model, and normalization pipeline matter so much. They let you absorb inconsistency at the edge and keep workflow logic stable in the core.
Embedding Security and Regulatory Compliance
Security retrofits usually reveal design errors that were already in production. The workflow runs, but the team cannot prove who approved a change, which policy applied, what data triggered an action, or whether access was valid at that moment. In healthcare, those gaps create audit exposure, patient safety risk, and expensive rework.
The fix is architectural. Compliance has to exist in the control plane, the data plane, and the operational model from day one. That means identity is enforced at service boundaries, approvals are part of workflow state, and audit records are generated as system outputs, not left to application logs.
Effective healthcare operations automation requires governance to be embedded at the design phase, including role-based access, segregation of duties, approval policies, and audit trails to prevent policy exceptions and support compliance audits (governance in healthcare operations automation architecture). Teams that treat these controls as backlog items usually end up rebuilding core services after security review.
Security by design changes the system shape
A compliant architecture has a different shape than a fast prototype. User identity should come from a central IdP such as Okta, Microsoft Entra ID, or Auth0. Service-to-service authentication should use short-lived tokens or workload identity, not shared API keys in configuration files. Authorization should be handled through policy services or gateway enforcement, with clear mappings between user role, workflow step, tenant boundary, and permitted action.
Approval logic also belongs in the domain model. If a prior authorization workflow requires a clinician review above a risk threshold, that checkpoint should be expressed as explicit workflow state with approver identity, timestamp, reason code, and immutable history. Audit evidence is much easier to defend when it is modeled this way.
The controls to define early are predictable:
Role-based access control: Map permissions to job function and workflow responsibility.
Segregation of duties: Separate request entry, approval, override, and execution where policy requires it.
Approval policies: Enforce step-up review for high-impact actions, exceptions, and overrides.
Audit trails: Capture user, service, action, timestamp, object changed, prior value, and resulting state.
Retention and change management: Keep records for the required period and tie every configuration change to an owner, ticket, and deployment record.
Practical controls that hold up in production
Encryption at rest and in transit is baseline engineering. Production failures usually happen elsewhere. A background job runs under a broad service account. An operations admin can view data across tenants. A rules engine can auto-close a case that policy says needs human sign-off. Those are architecture problems, not missing checkboxes.
I use a simple review frame during design and release readiness:
| Control area | What to verify |
|---|---|
| Identity | Are users, services, and scheduled jobs authenticated through managed identity instead of shared credentials? |
| Authorization | Can the team prove why access was granted at the exact time of the action? |
| Auditability | Are business events and security events stored in a form investigators and auditors can query without custom log recovery? |
| Workflow control | Do sensitive automations stop for approval, dual review, or exception handling where policy requires it? |
Security maturity shows up in workflow behavior.
Teams hiring for this work often underestimate how much architecture and compliance knowledge overlap. For a practical industry view of HIPAA skill requirements for cybersecurity, it helps to see how employers describe the mix of technical controls, risk management, and regulatory knowledge they expect.
Regulated SaaS product development also changes the platform design. Multi-tenant isolation, tenant-scoped audit logs, delegated administration, key management, data retention policy, and environment separation need to be built into the platform itself. They cannot be patched in per customer. The same discipline applies to AI-enabled workflows. Models that influence routing, prioritization, or recommendations need the same approval, traceability, and release controls as the application services around them. Our guide to machine learning models in healthcare software covers the model-specific controls teams should add on top of standard application security.
Integrating AI and MLOps Lifecycles
AI in healthcare automation needs a stricter operating model than standard software features. A model can degrade even when the application code is unchanged. Data drifts. Clinical practice changes. Documentation behavior shifts. Staff begins using the workflow differently. If the architecture doesn't track those changes, the model becomes a hidden liability.
That's why MLOps matters. Think of it as CI/CD for models, with stronger validation, more lineage, and more operational oversight.
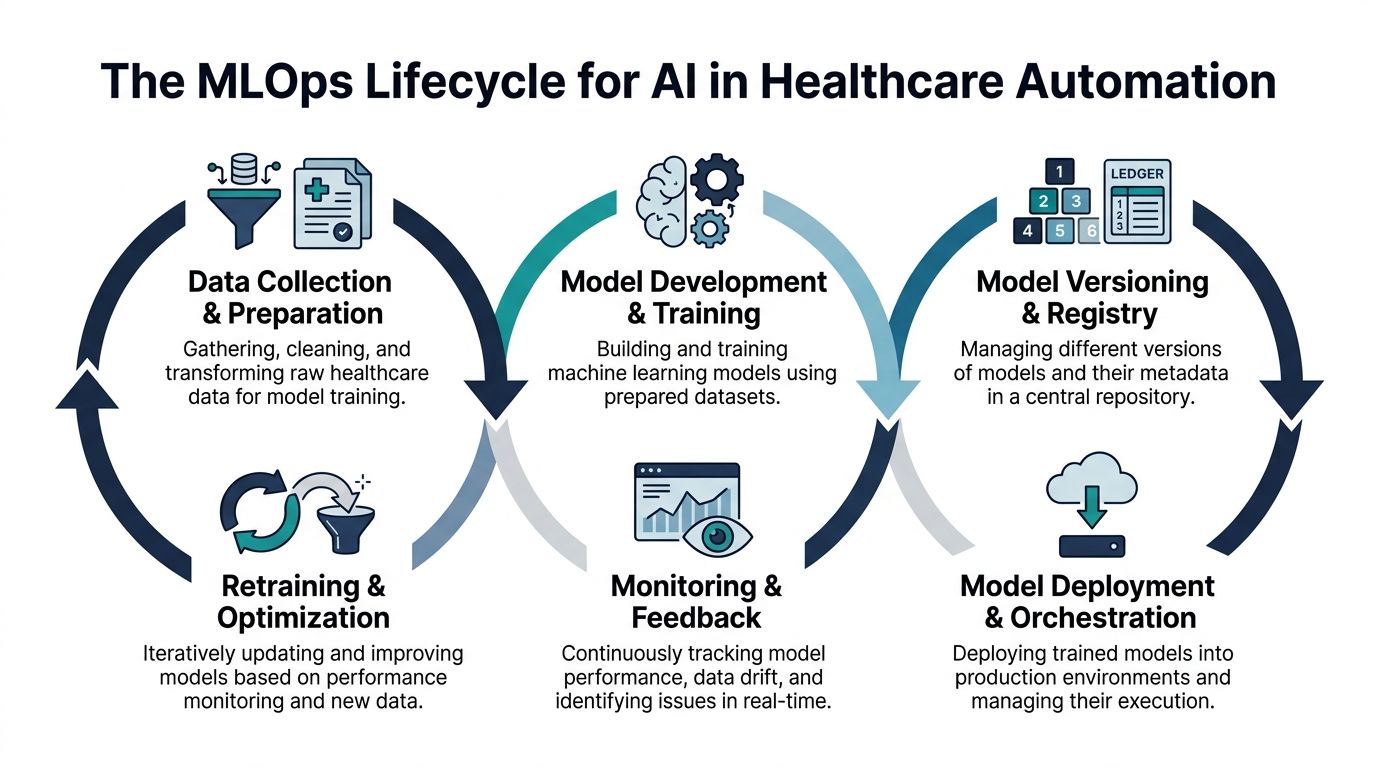
The production lifecycle that actually works
A usable model pipeline in healthcare needs more than training and deployment. It needs a managed chain from data preparation to retraining, with validation gates and rollback options.
I'd structure it like this:
Data preparation with governed datasets, versioned features, and documented inclusion rules.
Training and validation with performance checks tied to intended workflow use, not just generic benchmarks.
Model registry and release control so approved versions are explicit.
Serving and orchestration through isolated endpoints or model services that can be monitored independently.
Monitoring and feedback for drift, usage anomalies, and review outcomes.
Retraining or rollback when quality or policy thresholds are no longer met.
A good overview of production considerations appears in our guide to healthcare machine learning models, especially around the handoff between model output and operational workflow.
Keep AI behind workflow controls
One of the strongest patterns for healthcare AI agents is a hybrid flow. The system ingests a trigger event, pulls relevant unstructured context from the EHR, passes that context to the model, generates a draft output, and routes it to a human for review and sign-off before final action. That pattern is especially important in clinical and quasi-clinical workflows where risk tolerance is low.
What doesn't work is treating the model as the workflow engine. Models should assist classification, extraction, summarization, or drafting. Workflow engines should handle sequencing, routing, approvals, and exception logic.
If a model output can trigger an irreversible action, the review boundary must be visible in the architecture.
MLOps also affects workforce design
Teams often discuss AI architecture only in technical terms, but operating models change too. Reviewers, clinical SMEs, compliance teams, and data stewards all become part of the lifecycle. That's one reason healthcare organizations are rethinking specialist roles and responsibilities around AI-enabled processes. The broader talent shift is reflected in discussions about how AI transforms healthcare hiring.
For delivery teams, the practical stack usually includes model registries, feature stores where appropriate, containerized serving, workflow engines, observability tooling, and explicit policy checks around human review. Organizations that need implementation support often combine internal platform teams with external AI development services or broader enterprise AI solutions when the scope extends beyond a single workflow.
Implementation Checklists and Migration Paths
Analysts at McKinsey found that payer automation programs can produce first-year returns of 30 to 200 percent, with some operational workflows reaching break-even in 3 to 6 months (automation at scale in healthcare payers). That upside is real, but only when teams implement in the right order. In production, architecture mistakes usually show up as rework around data ownership, workflow state, and exception handling.
Greenfield versus brownfield
The first decision is usually structural. Build net new, or wrap and replace what already exists.
A greenfield approach fits new digital products, carved-out business units, or cases where legacy constraints would dictate the wrong architecture from day one. It gives the team cleaner domain boundaries, simpler contracts, and fewer hidden dependencies. The trade-off is organizational, not just technical. Teams often overbuild platforms before the workflow volume or adoption pattern is proven.
A brownfield approach is the default for providers, payers, and multi-entity health systems. Core EHR, billing, claims, and reporting platforms remain in place while new orchestration, adapters, eventing, and workflow services are added around them. Delivery is less tidy, but it lowers clinical and operational disruption. For many CTOs, that is the right trade.
| Path | Best fit | Main risk | Strong pattern |
|---|---|---|---|
| Greenfield | New products and major platform resets | Platform scope grows faster than business demand | Start with one bounded domain and add services only after usage proves the need |
| Brownfield | Enterprise modernization with entrenched source systems | Legacy coupling leaks into every new service | Put APIs, adapters, and orchestration in front of legacy systems before replacing internals |
For brownfield modernization, the safest migration path is usually incremental. A strangler-pattern approach to legacy healthcare system migration to cloud lets teams move one capability at a time while preserving system continuity, auditability, and user adoption.
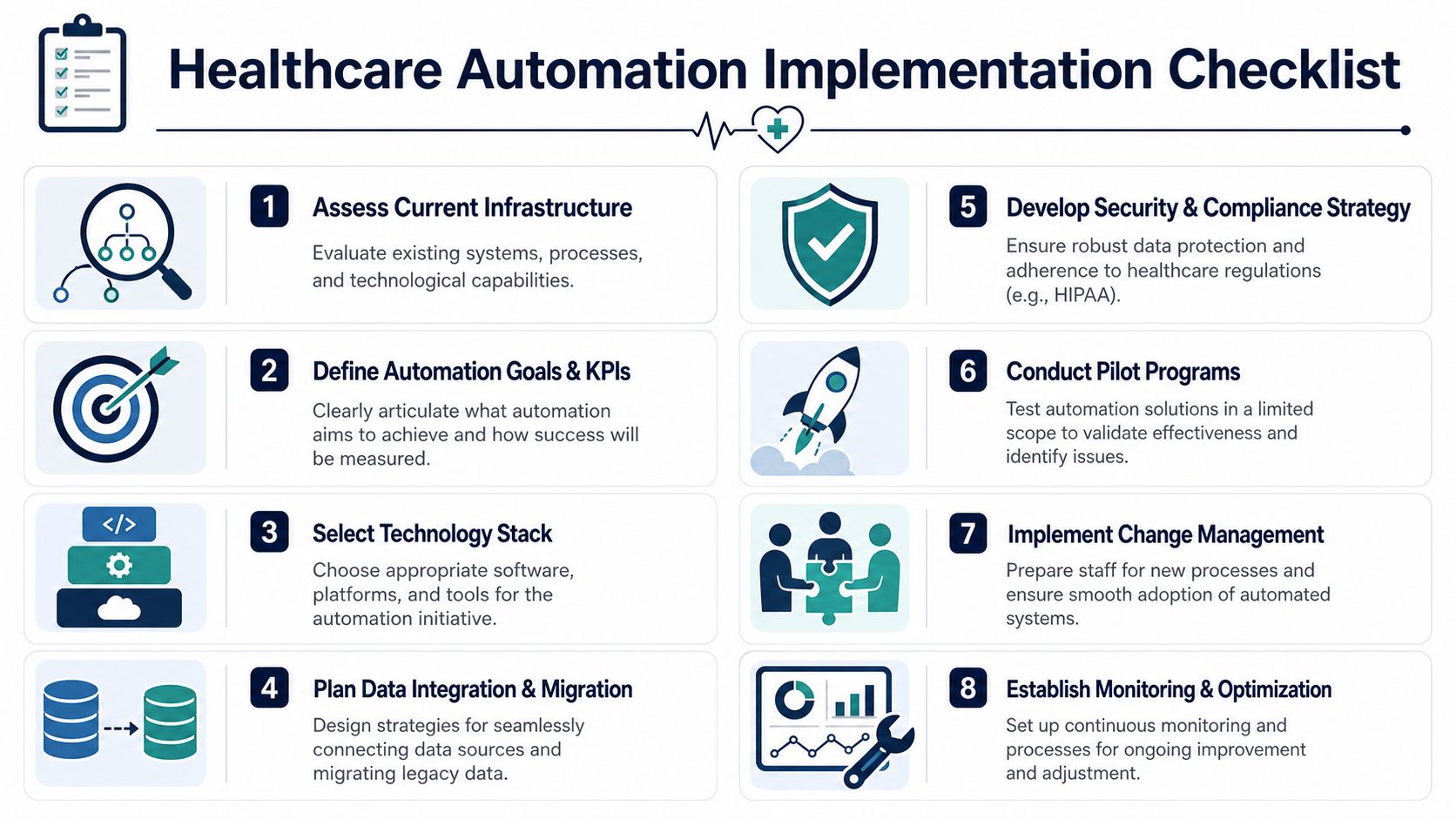
A practical implementation checklist
Teams that succeed usually start narrower than they planned.
Use this sequence:
Map one workflow end to end: Choose a bounded process such as intake, prior authorization support, or billing follow-up. Capture source systems, approvals, exception cases, manual workarounds, and service-level targets.
Assign system ownership by domain: Identify the system of record for patient, encounter, authorization, claim, task, and document data. If two systems write to the same field, define reconciliation rules before go-live.
Define canonical contracts early: Standardize event names, payload schemas, correlation IDs, and idempotency behavior. This prevents each integration team from inventing its own pattern.
Choose orchestration deliberately: Use a workflow engine for long-running state, retries, timers, escalations, and approvals. Use direct service calls only for short, deterministic transactions.
Isolate unavoidable legacy interaction: If a critical system still requires screen automation, keep RPA behind APIs or task workers so bots do not become the process controller.
Design review operations as part of the product: Build queues, triage states, assignment rules, and audit trails early. Human review paths determine whether the workflow is safe to scale.
Instrument the workflow before expansion: Capture technical telemetry and business metrics from the first pilot. Teams need latency, failure rates, queue age, rework volume, and completion time by exception type.
Pilot one domain, then widen scope: Prove that exception handling, support ownership, rollback procedures, and reporting work under live conditions before adding adjacent workflows.
Technology choices that hold up in production
The best stack is the one your team can operate under audit, during incidents, and across vendor changes.
A sensible baseline usually looks like this:
Cloud and runtime: AWS, Azure, or Google Cloud. Use containers, managed identity, secrets management, and infrastructure-as-code.
API and interoperability layer: FHIR services where they fit, API gateways, interface engines, and custom adapters for systems that do not expose usable standards.
Messaging backbone: Kafka, RabbitMQ, or managed event buses for asynchronous updates, decoupled consumers, and replayable event flows.
Workflow engine: Camunda, Temporal, or a similar engine when the process has approvals, waits, retries, and state transitions that matter to operations.
Data stores: Transactional databases for workflow state, object storage for documents, and analytics stores separated from operational workloads.
Observability and audit: Centralized logging, traces, metrics, alerting, immutable audit events, and dashboarding tied to workflow KPIs.
The build-versus-partner question also belongs here. Some organizations have the internal platform maturity to assemble and run this stack themselves. Others need outside delivery help for integration-heavy or regulated workloads. In those cases, custom software development, flexible service models, or product-focused SaaS engineering are delivery decisions tied to architecture, staffing, and support ownership. Bridge Global is one example of a delivery partner used for that mix of healthcare engineering, integration work, and AI implementation support.
Frequently Asked Questions
What's the best first use case for healthcare automation architecture?
Start with a workflow that fails often, eats staff time, and has clear decision rules. Patient intake, prior authorization support, billing follow-up, and claims operations usually fit better than clinician-facing decision automation in phase one. They generate enough volume to test queueing, retries, exception handling, audit trails, and handoffs without putting the highest-risk clinical controls in the first release.
A good first use case also has a measurable baseline. Time to complete, rework rate, manual touches, and denial rate are better starting metrics than broad transformation goals.
Can a legacy EHR stay in place while the automation platform evolves?
Yes. In production, that is the standard path.
Most healthcare teams cannot replace the EHR and redesign operations at the same time without creating delivery and compliance risk. The safer pattern is to keep the EHR in place, wrap it with integration services, and move orchestration into systems your team can version, test, and monitor. That gives product and engineering teams room to improve workflows in stages while keeping the system of record stable.
When should teams use RPA instead of APIs?
Use APIs when the source system exposes a stable interface with acceptable governance and support. Use RPA when a system has no practical API, the workflow still matters, and the cost of manual work is high enough to justify the maintenance burden.
RPA should stay at the edge. Put orchestration, business rules, audit logging, and exception routing in services you control. If the bot becomes the process brain, every UI change turns into an incident.
How much AI should be in the first release?
Keep the first release narrow. AI works well early for document classification, summarization, extraction, draft generation, and queue prioritization where a human reviewer stays in the loop. That approach helps teams prove value while collecting the operational data needed for model monitoring, prompt review, and policy enforcement.
Do not put core workflow state or approval logic inside a model. Keep those decisions in deterministic services, rule engines, and workflow definitions.
What's the most common architecture mistake?
Teams automate a task and call it architecture.
The failure usually shows up six months later. Point-to-point connections multiply, data definitions drift by system, exception paths live in inboxes, and audit evidence is incomplete when compliance asks for it. The fix is boring but effective. Define canonical business events, assign system ownership, make approval boundaries explicit, and design for retries and reconciliation before scaling to the next workflow.
How do product leaders evaluate implementation partners?
Ask implementation questions, not sales questions. Which interoperability standards have they shipped in healthcare environments? How do they test workflow changes before release? What is their pattern for PHI isolation, access control, audit retention, and AI review? Who owns runbooks, support handoff, and incident response after go-live?
Past delivery evidence matters. Reviewing relevant client cases is a reasonable way to check whether a partner has handled integration-heavy and regulated product work similar to yours.
Bridge Global works with healthcare teams building regulated platforms, operational automation, and AI-enabled systems. If you need a practical architecture and a delivery team that can handle phased modernization, integration work, workflow services, and model operations, Bridge Global is one option to evaluate.
About Upendra Jith
Upendrajith completed his Master's in English and has been a commercial content developer for the past three years. He's more inclined to develop content with a 'street-smart' delivery on topics such as technology, media, or anything he can get his hands on. He has a fixation on lyrics, dark poetry, media, technology, and flow arts.
View all posts by Upendra Jith →