


Legacy Healthcare System Migration to Cloud: A Guide
Your hospital is probably in a familiar bind. Core systems still run. Clinicians know their workarounds. Finance knows which batch jobs must never fail. But every change takes too long, every integration feels brittle, and every security review exposes another piece of aging infrastructure that no one wants to touch.
That’s why legacy healthcare system migration to cloud can’t be treated as a simple hosting move. In healthcare, you’re not just relocating applications. You’re preserving care delivery, protecting regulated data, and keeping interfaces alive while old and new systems run together.
The most successful migrations I’ve seen start with a sober premise: the cloud is useful, but it doesn’t forgive vague planning. It rewards clear sequencing, hard decisions about what to keep, and disciplined control over interoperability, access, and cost. By 2024, healthcare modernization priorities had clustered around EHRs, cybersecurity, digitization, and virtual care, with one industry study cited by BGO Software reporting that these areas consumed 85% of surveyed organizations’ digital and technology budgets (healthcare modernization priorities). That tells you where the stakes are. This is now an operational program, not a side IT project.
The Foundation for a Successful Cloud Migration
A migration usually fails long before the first workload moves. It fails in discovery when the organization underestimates dependencies, ignores workflow exceptions, or treats every application as equally important.
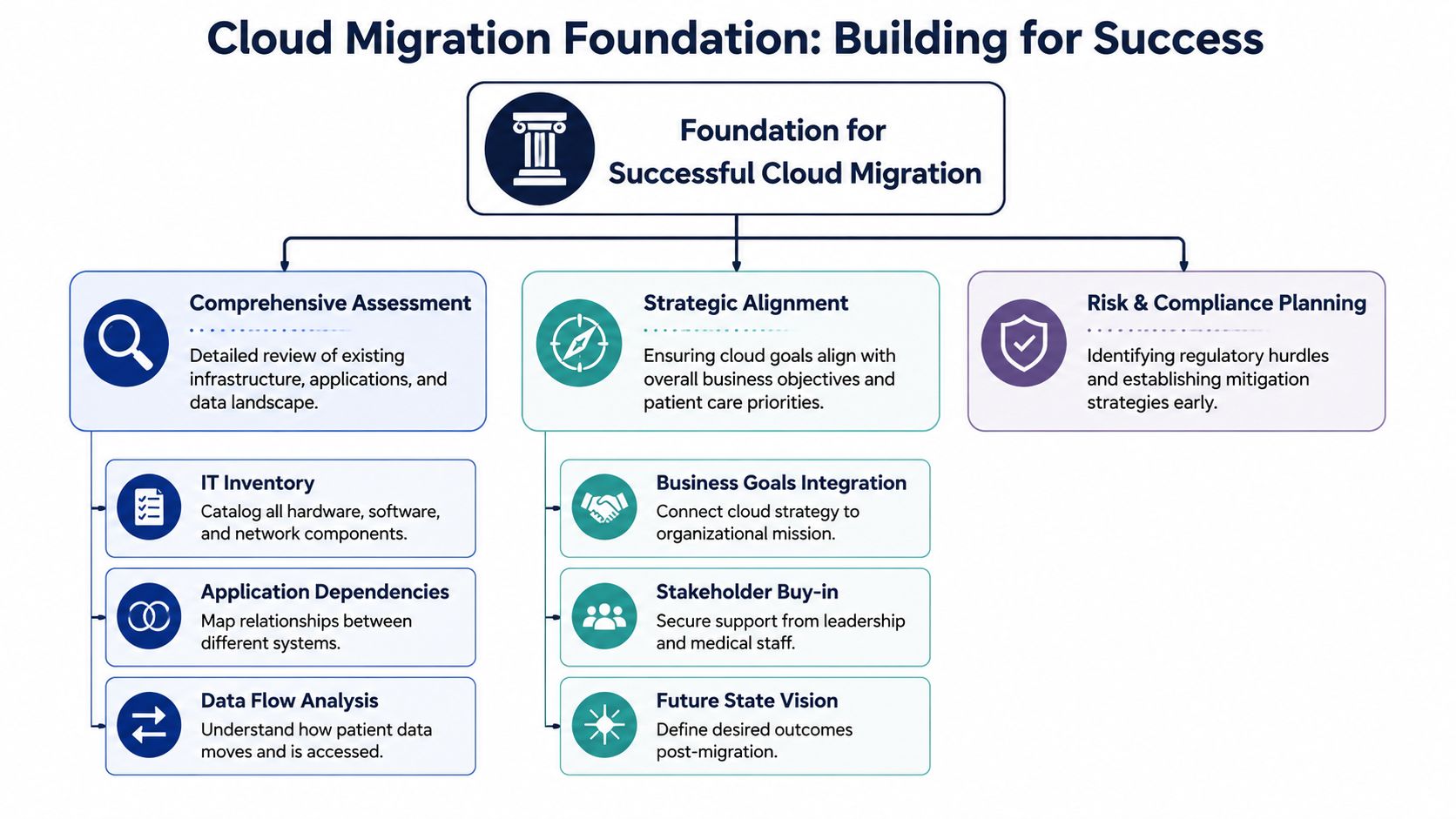
Start with service lines, not servers
Don’t begin with an infrastructure inventory alone. Start with care and business capabilities. List the functions the hospital cannot interrupt: inpatient documentation, results routing, admissions, identity, billing, imaging access, pharmacy coordination, and clinician authentication.
Then map systems to those functions:
-
Clinical systems: EHR, EMR modules, PACS, LIS, RIS, patient portal
-
Operational platforms: scheduling, ERP, revenue cycle, HR, supply chain
-
Shared control points: Active Directory or equivalent identity systems, interface engines, audit logging, reporting stores
That changes the conversation. Instead of asking, “What can we move first?” you ask, “What can move without breaking a clinical or revenue workflow?”
For organizations planning broader modernization, this is where custom healthcare software development becomes relevant. Some systems can be migrated as they are. Others need targeted replacement, integration work, or workflow redesign before they’re safe to move.
Build a cloud-readiness score that reflects reality
I recommend scoring each application against a short set of practical criteria.
-
Dependency density
Count how many upstream and downstream systems it touches, including authentication, HL7/FHIR flows, reporting extracts, and batch jobs. -
Data sensitivity
PHI, billing data, operational logs, and image archives don’t carry the same migration risk. -
Downtime tolerance
A departmental admin tool may accept a maintenance window. A medication or order workflow may not. -
Technical debt
Old OS versions, unsupported middleware, hardcoded file paths, and undocumented interfaces all increase migration friction. -
Recovery posture
If rollback is needed, can the team restore service cleanly?
Practical rule: Move a low-risk but useful workload early. Don’t start with the noisiest system in the estate just because it’s old.
A sound discovery phase also includes data flow diagrams, interface ownership, archive obligations, and vendor constraints. Procurement and architecture teams should work together here. A useful companion resource is this guide to vendor evaluation for cloud solutions, especially when comparing support models, contractual boundaries, and operational fit.
Secure buy-in before design hardens
A CTO can approve architecture. That doesn’t mean the migration has organizational support. You need a sign-off from clinical operations, compliance, security, integration owners, and finance before wave planning gets locked.
The practical output from this phase should be small and clear:
-
A migration scope with in-scope and deferred systems
-
A business-ranked application list based on value and risk
-
A dependency map that integration teams accept
-
A target operating model for support, ownership, and escalation
If those four artifacts are weak, the project will drift.
Navigating the Healthcare Compliance and Risk Minefield
In healthcare, architecture decisions become compliance decisions very quickly. A storage bucket, a logging setting, or an overly broad IAM role can create exposure that doesn’t show up until audit time or incident response.

One healthcare modernization report stated that more than 276 million patient records were compromised in 2024 (reported record compromises in 2024). That figure is a blunt reminder that migration planning has to start with risk controls, not convenience.
Classify data before you classify workloads
Many teams classify applications first. That’s backwards. Classify the data they handle first:
-
Protected health information
-
Financial and billing records
-
Operational and scheduling data
-
Audit logs and security telemetry
-
Research or analytics datasets
Once data classes are defined, map each class to control requirements. That includes encryption, retention, access boundaries, auditability, and approved transfer paths. If a cloud service can’t meet the required control set for the data it will hold or process, it doesn’t belong in the target design.
Understand the shared responsibility line
Cloud platforms don’t remove accountability. They change where technical responsibility sits. The provider secures the underlying platform components they own. Your team still has to configure identity, access, logging, segmentation, key handling, backup policy, and workload-level controls correctly.
That’s where many first migrations struggle. Teams assume a compliant cloud service automatically means a compliant deployment. It doesn’t.
A practical operating checklist should include:
-
Least privilege by default: No broad administrator access for migration convenience
-
Encrypted data paths: Especially for bulk transfer, replication, and temporary staging
-
Centralized logging: Logs from network, identity, application, and database layers in one reviewable stream
-
Documented exceptions: Every control gap during transition needs an owner and an expiry date
For teams tightening governance, a structured roadmap for secure HIPAA compliance can help frame monitoring, evidence collection, and control verification in a cloud context.
Compliance breaks most often in the seams between systems, teams, and handoffs. That’s why migration governance has to include integration paths, temporary storage, and support access, not just the final production design.
Design for auditability, not just protection
Security architecture that can’t be explained is hard to defend. During migration, every temporary bridge matters: replication tools, ETL pipelines, cutover scripts, masked test data, and fallback environments.
I advise CTOs to require three forms of evidence from day one:
| Evidence type | What to capture | Why it matters |
|---|---|---|
| Control evidence | IAM policies, encryption settings, approved network paths | Supports audit and internal review |
| Migration evidence | test results, validation sign-offs, rollback criteria | Shows due diligence during transition |
| Operational evidence | alerting, access logs, incident workflows | Proves the environment can be governed after go-live |
If you need a deeper governance reference for regulated delivery, Bridge Global has a whitepaper on digital health speed and compliance that's relevant to cloud-era delivery controls.
Choosing Your Migration Path for Healthcare Systems
A healthcare portfolio never moves with one migration pattern. Trying to force one approach across all systems usually creates either unnecessary cost or unnecessary risk.
A practical migration methodology in healthcare follows a five-phase sequence of assessment and strategy, provider selection, data-migration planning, implementation, and optimization/support, while choosing the right pattern per component, such as rehost, replatform, refactor, replace, or retire before pilot testing and final cutover (five-phase healthcare migration methodology).
The decision lens that works in hospitals
I use four filters when choosing a pattern:
-
Clinical criticality: If failure disrupts care delivery, choose the safest path first
-
Integration fragility: The more brittle the interfaces, the less appetite you have for big change during early waves
-
Change horizon: If the system will be replaced soon, don't over-engineer its cloud target state
-
Strategic value: If the platform must support analytics, APIs, or AI later, shallow migration may create technical drag
That's why lift-and-shift isn't always lazy. In healthcare, it can be the safest bridge for mission-critical systems while the organization stabilizes interfaces, observability, and governance.
Comparing the 6 R's of Cloud Migration for Healthcare
| Strategy | Description | Best For | Risk Level |
|---|---|---|---|
| Rehost | Move the application largely as-is to cloud infrastructure | Stable legacy apps where speed and low change are priorities | Medium |
| Replatform | Make limited platform changes without major code redesign | Apps needing better manageability, backup, or database support | Medium |
| Refactor | Redesign the application for cloud-native architecture | Patient-facing platforms, API-heavy services, growth systems | High |
| Repurchase | Replace with a SaaS or packaged platform | Outdated systems where product fit is stronger than rewrite economics | Medium to High |
| Retire | Decommission redundant or unused components | Duplicate reporting tools, dead interfaces, obsolete portals | Low |
| Retain | Keep on-premise or defer migration for now | Systems blocked by contract, compliance, latency, or integration timing | Low to Medium |
What works and what doesn't
What works:
-
Rehost first for tightly coupled legacy applications when uptime matters more than elegance
-
Replatform middleware and databases selectively if that improves supportability without rewriting core logic
-
Refactor only where there's a clear future payoff, such as APIs, patient self-service, or scalable remote care
What doesn't:
-
Refactoring under deadline pressure, while the hospital also expects zero operational disruption
-
Repurchasing without workflow fit analysis, especially in revenue cycle and specialty clinical areas
-
Retaining too much by default, which leaves you funding both estates indefinitely
For organizations that need implementation help across hosting, security, and modernization planning, cloud services can support the transition model, but the architecture choice still has to be made system by system.
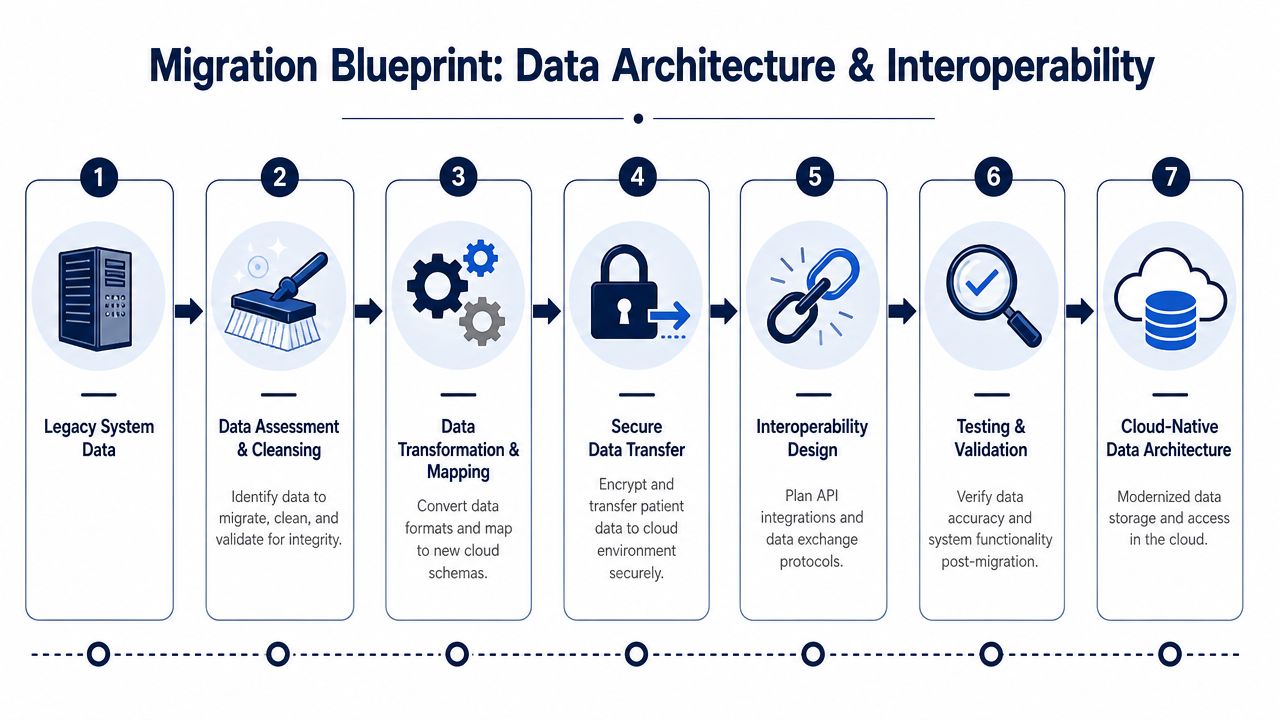
The Migration Blueprint Data Architecture and Interoperability
Most migration plans look clean until the first interface fails. Then everyone remembers that the hospital doesn't run on applications alone. It runs on message flows, identity relationships, and data timing.
InfoQ notes that EMR integration is costly and challenging, and that observability must be prioritized in microservices-based migrations. That's why a phased migration often becomes an interoperability program first, infrastructure program second (operational continuity and EMR integration challenge).
Preserve continuity in a hybrid state
During transition, some systems will remain on-premises while others move to cloud services. That hybrid state is where many avoidable incidents happen.
The target architecture should explicitly define:
-
System of record ownership
Decide which system is authoritative for each data domain during each migration wave. -
Interface behavior during dual operation
Clarify whether messages are mirrored, routed, transformed, queued, or replayed. -
Identity and access continuity
Keep clinicians from seeing different login behavior across old and new platforms unless there's a deliberate cutover plan. -
Operational observability
Monitor transaction success, queue depth, latency, and data mismatches across both environments.
If your EHR, lab, and billing teams can't answer who owns a patient update during wave two, you aren't ready for wave two.
Treat data migration as mapping, validation, and reconciliation
Healthcare data isn't just rows to copy. Codes, attachments, images, free text, historical records, and audit trails all carry different business value and regulatory weight.
A practical sequence looks like this:
-
Assess and cleanse: Remove duplicates, flag incomplete records, resolve stale mappings
-
Transform and map: Align source fields to the target model and document exceptions
-
Transfer securely: Use approved, encrypted paths and controlled staging
-
Validate and reconcile: Confirm record accuracy, interface behavior, and workflow usability
FHIR and API-led design can help, especially for future-facing interoperability, but they won't erase legacy complexity by themselves. Hospitals still need careful mapping between old schemas, integration engines, and target services.
Build the bridge before you remove the old road
This is where modern healthcare integrations matter. Integration layers, interface engines, API gateways, event routing, and reconciliation jobs should be designed as first-class migration assets, not temporary plumbing.
If you've ever seen a phased migration unravel, it usually wasn't because compute failed. It was because admissions stopped receiving updates, a result feed arrived late, or a billing dependency nobody documented surfaced on the go-live weekend.
Go-Live Cutover Testing and Cost Optimization
Go-live is a controlled risk event, not a celebration point. The teams that do this well treat cutover, rollback, and post-launch cost management as one continuous operating motion.
The economics matter too. Many articles argue that cloud migration improves efficiency, but they don't quantify the total cost of ownership or hidden costs, which is why healthcare leaders have to test whether migration reduces cost versus shifting it elsewhere (cost efficiency and hidden cost gap).
Test the workflow, not just the platform
A workload can pass infrastructure checks and still fail the hospital. Technical testing has to include operational reality.
Run at least these layers:
-
Functional testing: Core workflows, interfaces, report generation, and user roles
-
Performance testing: Peak clinical usage, batch windows, document retrieval, concurrent sessions
-
Security testing: Access boundaries, logging, privileged workflows, secrets handling
-
User acceptance testing: Clinician, admin, and revenue-cycle scenarios that reflect real-day-to-day use
I always push for scripted scenarios from actual departments. “Patient admitted, lab ordered, result posted, discharge processed, bill generated” is far more useful than abstract pass/fail testing.
Your cutover plan needs a rollback threshold
A serious cutover runbook has named owners, exact decision points, communication trees, and a clear rollback trigger. Not a vague promise to “revert if needed.”
Use a short command structure:
| Cutover item | Owner | Decision point |
|---|---|---|
| Data freeze | application lead | source updates paused and confirmed |
| Final sync | data team | reconciliation accepted |
| Interface switch | integration lead | test messages validated |
| User access change | IAM lead | role mapping confirmed |
| Rollback gate | executive and technical leads | proceed or revert based on predefined criteria |
A rollback plan is only real if the team has tested it under time pressure.
Control spend from the first billing cycle
Cloud overspend usually starts with good intentions. Extra environments stay online. Storage tiers aren’t reviewed. Logging grows without retention discipline. Lifted workloads carry old sizing assumptions into a metered platform.
FinOps in healthcare should focus on:
-
Tagging and ownership: Every resource tied to a department, workload, or project
-
Rightsizing: Adjust compute and database configurations after real production patterns appear
-
Environment lifecycle controls: Shut down nonproduction resources when they aren’t needed
-
Observability budgets: Keep useful logs, but define retention by risk and compliance need
For delivery partners handling migration engineering or modernization follow-on work, custom software development, and published client cases can be useful references when evaluating implementation depth and post-go-live support models.
The Future-Ready Cloud Governance and AI Enhancements
A hospital doesn’t get strategic value from migration just because workloads now run in the cloud. Value appears when the cloud estate is governed well enough to support change without introducing new instability.
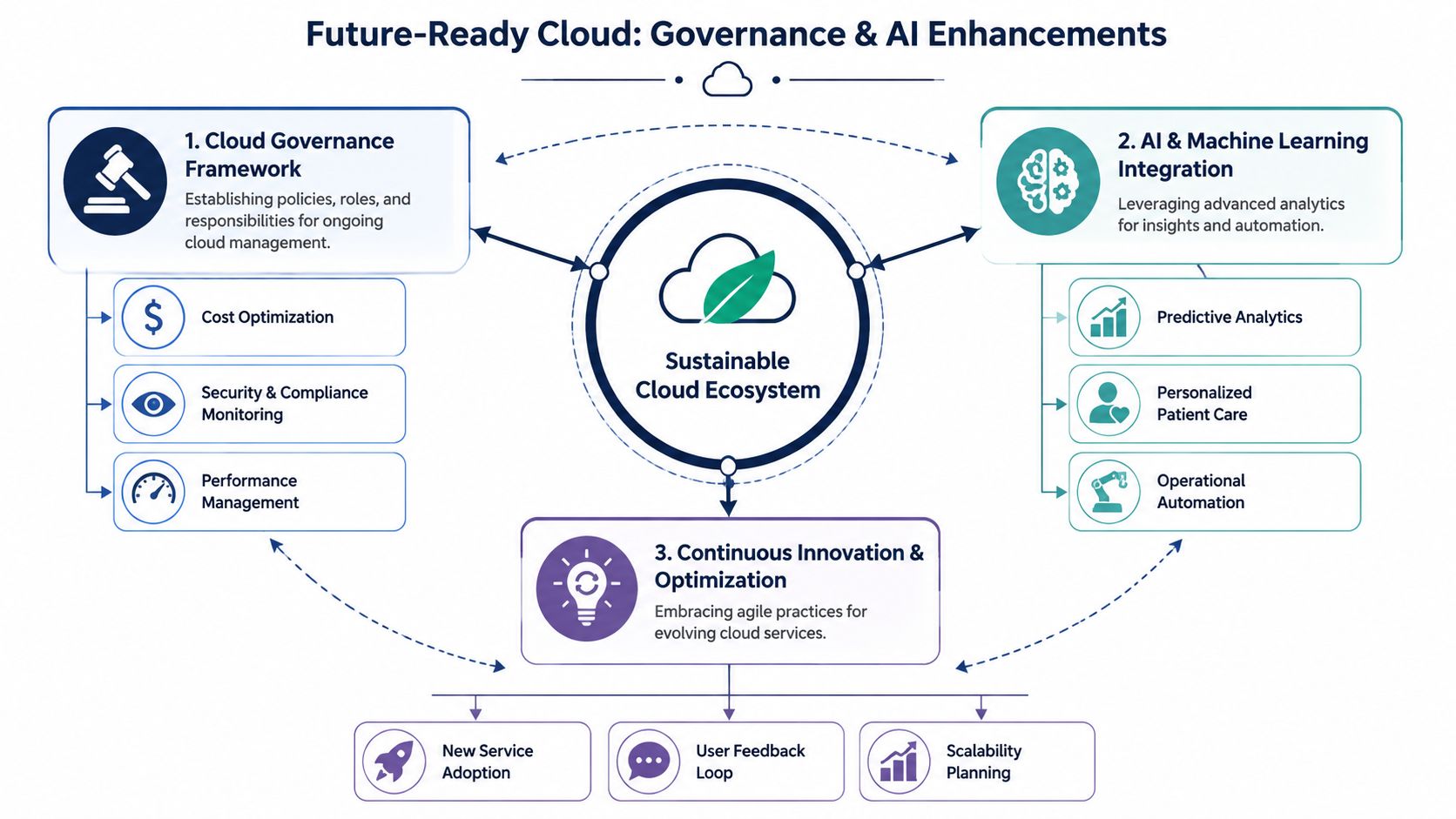
Put governance in place before innovation accelerates
Most healthcare organizations need a lightweight but real cloud governance model:
-
A cloud decision forum: Architecture, security, compliance, and operations reviewing major changes
-
Standard landing patterns: Approved templates for networking, IAM, logging, storage, and backup
-
Operational accountability: Named owners for resilience, patching, performance, and spend
-
Continuous monitoring: Not just security alerts, but service health, integration quality, and policy drift
This is also where partner selection matters. A healthtech software development partner should be able to work inside those controls, not around them.
AI readiness depends on migration discipline
Healthcare leaders often ask when AI enters the picture. The answer is after identity, data quality, interoperability, and governance are stable enough that AI workloads won’t amplify noise.
Useful next steps often include:
-
Predictive and operational analytics built on governed data pipelines
-
Workflow automation for admin-heavy processes and triage support
-
Scalable patient-facing services that use cloud-native APIs and event-driven architecture
-
Model-enabled products delivered through AI development services or broader enterprise AI solutions
If the roadmap includes AI, plan it intentionally. An AI implementation roadmap helps connect governance, data readiness, and use-case selection so the migration becomes a platform for measured innovation instead of a disconnected infrastructure project.
Don’t let modernization stop at hosting
Some healthcare platforms should evolve beyond infrastructure migration into product thinking. Patient access tools, remote care platforms, specialty workflows, and partner portals often benefit from a more productized architecture and, in some cases, from SaaS product development.
As we explored in our guide to healthcare modernization and integration strategy, the cloud only fully realizes its potential when governance, delivery discipline, and data architecture mature together.
Frequently Asked Questions About Healthcare Cloud Migration
How should a hospital decide what to migrate first?
Start with systems that are important enough to matter but safe enough to learn from. Good first candidates usually have limited downstream dependencies, manageable downtime windows, and clear operational ownership. Avoid beginning with the most politically sensitive or integration-heavy clinical platform unless there’s a hard business reason.
Is lift-and-shift a bad strategy in healthcare?
No. It’s often a sensible first step. For tightly coupled legacy systems, rehosting can reduce infrastructure risk without forcing application redesign during a fragile transition period. The mistake is stopping there for systems that later need better scalability, interoperability, or product evolution.
How do we protect clinical operations during phased migration?
Treat the hybrid period as a formal target state, not a temporary inconvenience. Define data ownership by wave, monitor interfaces aggressively, rehearse fallback procedures, and make sure clinical teams know exactly what changes and what doesn’t. Parallel operations can be awkward, but they’re often safer than an all-at-once switch.
What usually causes migration budgets to drift?
Three things show up repeatedly: underestimated integration work, poor application discovery, and weak post-go-live cost controls. Budget pressure also rises when organizations carry old and new estates longer than planned or refactor too many systems at once.
Should we modernize applications before or after the move?
It depends on the system. If the application is stable and critical, move it with minimal change first. If the application is customer-facing, API-heavy, or central to future digital strategy, selective modernization before or during migration may be justified. The right answer is rarely uniform across the estate.
How much change management is really needed?
More than most CTOs expect. Migration affects clinicians, back-office teams, support staff, security teams, and vendors. Role-based training, cutover communications, support escalation paths, and fast issue triage are as important as infrastructure readiness. Technical success without user adoption still counts as a failure.
What should we expect after go-live?
Expect a stabilization phase. Teams will tune performance, resolve edge-case workflow issues, tighten IAM permissions, refine alert thresholds, and revisit cost assumptions. This isn’t a sign that the migration went badly. It’s part of taking a live healthcare workload from operational to dependable.
If you’re planning legacy a healthcare system migration to the cloud and need a delivery team that can work across compliance, interoperability, modernization, and AI readiness, Bridge Global is one option to evaluate. Their work spans healthcare engineering, cloud enablement, product development, and AI-driven transformation, which makes them relevant for organizations that need both migration execution and a longer-term modernization path.
About Upendra Jith
Upendrajith completed his Master's in English and has been a commercial content developer for the past three years. He's more inclined to develop content with a 'street-smart' delivery on topics such as technology, media, or anything he can get his hands on. He has a fixation on lyrics, dark poetry, media, technology, and flow arts.
View all posts by Upendra Jith →