


Virtual Care Infrastructure: A Healthtech Blueprint
Telemedicine didn't become important because video got better. It became infrastructure because usage changed faster than most health systems could re-architect around it. In the first months of the pandemic, telemedicine encounters surged 766%, rising from 0.3% of all healthcare interactions in 2019 to 23.6% in the same period in 2020 in a national study of 36 million privately insured working-age individuals, with sustained elevation afterward in claims patterns (national study and FAIR Health discussion). That shift exposed a hard truth. Most organizations didn't have a virtual care strategy. They had a collection of tools.
That distinction matters now more than it did in the emergency phase. The virtual care market is projected to grow from USD 13.57 billion in 2024 to USD 114.85 billion by 2032, with a projected 29.27% CAGR, while online doctor consultation users reached over 116 million in 2024 (virtual care market projection). If you're building in this space, the question isn't whether virtual care is part of your operating model. The question is whether your architecture, governance, and delivery model can support it without becoming brittle, expensive, or exclusionary.
What Is Virtual Care Infrastructure
Virtual care infrastructure isn't a video feature inside a patient app. It's the operating grid that lets digital care run safely, repeatedly, and at enterprise scale.
The easiest way to think about it is this. A telehealth visit is the building. Virtual care infrastructure is the city grid underneath it: identity, connectivity, data movement, auditability, workflows, clinician tooling, patient access, storage, and operational controls. Leaders who treat virtual care as a front-end product decision usually end up rebuilding core services later under time pressure.

A virtual hospital model has three mandatory blocks: a patient application, a provider application, and a cloud server, working together with real-time video streaming and cloud-based EHR or PHI storage for consultation records and analytics. If one of those blocks is weak, the whole service degrades. If two are weak, clinicians start creating workarounds outside the system.
The application is visible. The infrastructure is decisive
Teams often overinvest in what patients can see and underinvest in what clinicians, operations, compliance, and finance need to trust. That's backwards.
A stable virtual care stack has to answer practical questions early:
-
Can patients start care without friction?
Scheduling, identity verification, consent, reminders, and fallback paths all matter.
-
Can clinicians deliver care without context switching?
If providers need multiple windows, duplicate charting, or manual handoffs, adoption stalls.
-
Can the business bill and audit correctly?
Modifier logic, claims integrity, encounter logging, and role-based access aren't side concerns.
-
Can the platform evolve?
If one SDK, one workflow assumption, or one vendor contract dictates your future roadmap, you don't have infrastructure. You have dependence.
Practical rule: If replacing one subsystem would break scheduling, documentation, billing, and communication at once, your platform is coupled too tightly.
For teams planning platform builds or modernization, choosing a healthtech software development partner matters because these systems cross product, compliance, data, and operations boundaries. This isn't just software procurement. It's service design under clinical and commercial constraints.
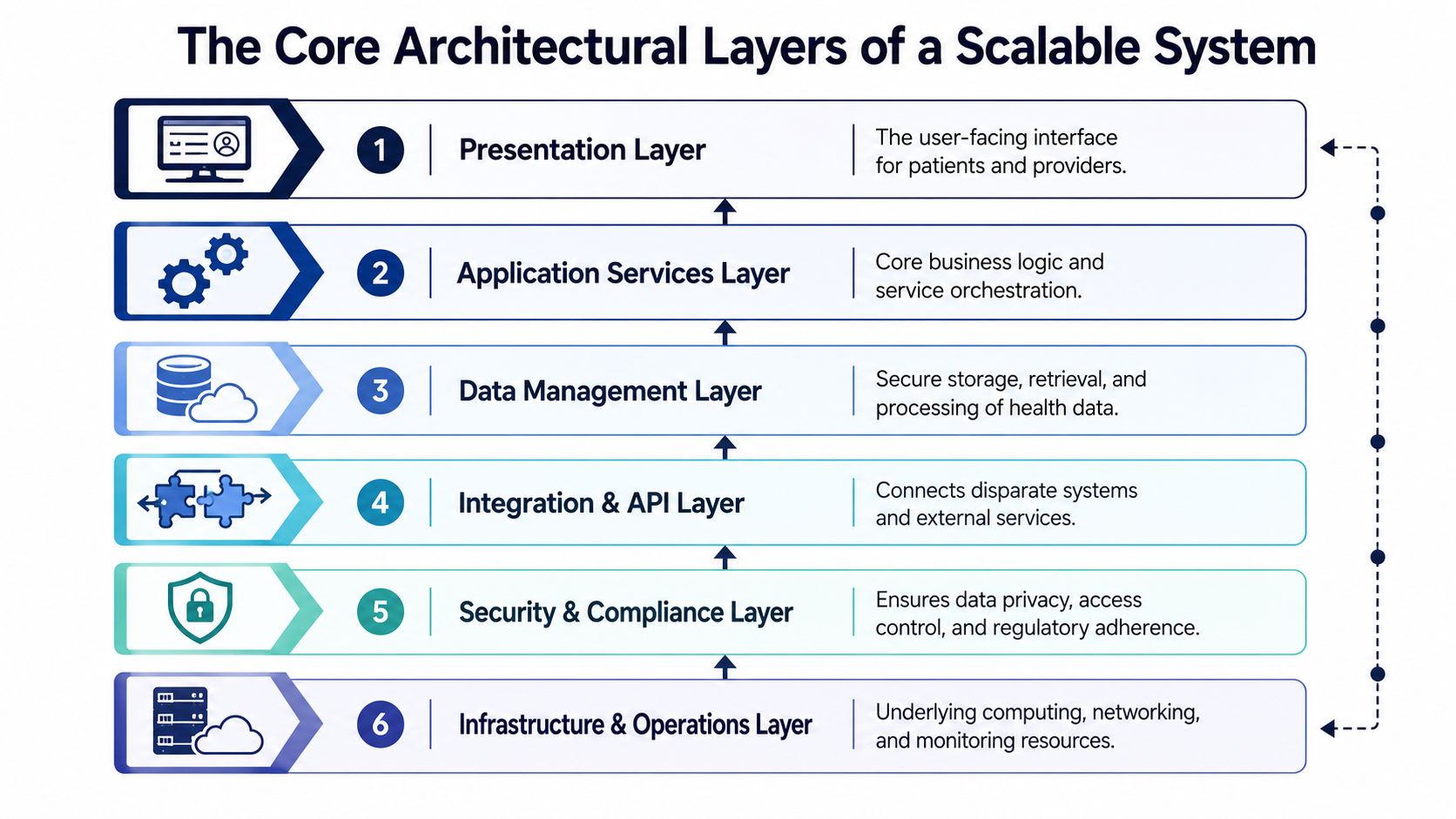
The Core Architectural Layers of a Scalable System
Scalable platforms don't emerge from a big feature list. They emerge from clear architectural separation.
A robust virtual care platform should be decomposed into six layers: Patient Engagement, Clinical Delivery, Clinical Intelligence, Revenue Cycle Operations, Analytics and Governance, and a Vendor-Agnostic Communication Architecture. Just as important, tying the product too closely to a single video SDK creates structural fragility.
Six layers that should stay distinct
Patient Engagement covers web and mobile scheduling, intake, reminders, consent, messaging, and asynchronous interactions. This layer should optimize for low friction and graceful failure. Patients don't care which backend service failed. They care that they couldn't join care.
Clinical Delivery is where synchronous visits, remote monitoring, virtual rounding, and provider workflows live. This layer needs to serve clinicians, not just compliance checklists. Fast note access, encounter controls, escalation paths, and device continuity matter more than visual polish.
Clinical Intelligence handles triage logic, risk stratification, and decision support. Many teams overpromise in this area. Keep intelligence modular. If triage rules, model outputs, and routing decisions can't be inspected or overridden, operations teams will stop trusting them.
What usually breaks first
The weak points are rarely the ones in demo flows. They show up in operational seams.
-
Revenue Cycle Operations: Telehealth modifier handling, claims scrubbing, and payer-specific logic need explicit services. If billing rules live inside scattered workflow code, maintenance gets expensive fast.
-
Analytics and Governance: Utilization tracking, audit logs, consent history, and exception monitoring need to be first-class capabilities. Retrofitting governance after launch is painful.
-
Vendor-Agnostic Communication Architecture: Keep communication services abstracted from the clinical core. A video vendor should be swappable without rewriting scheduling, documentation, and encounter logic.
Continuous data ingestion from wearables also belongs in the architecture discussion early. If remote monitoring data enters the platform as raw, unnormalized streams with no routing logic, clinical teams drown in noise instead of getting action-ready signals.
A practical implementation pattern is to keep user-facing applications thin and push business logic into stateless APIs and orchestration services. That creates room for replacement, testing, and phased upgrades. It also supports stronger healthcare platform API engineering when your roadmap includes EHRs, RPM devices, partner apps, or payer workflows.
Architect for substitution. Every major service should be replaceable without forcing a rewrite of adjacent layers.
For organizations investing in custom healthcare software development, this layered model is the difference between a platform that scales and one that accumulates hidden integration debt. Strong healthcare integrations don't start with connectors. They start with separation of concerns.
Ensuring Compliance Security and Interoperability
Compliance, security, and interoperability are often discussed as parallel workstreams. In practice, they're architectural constraints that shape the same system.
If your access model is loose, your compliance posture is weak. If your data contracts are proprietary, your interoperability story is weak. If your logs can't reconstruct who saw what and when, your security controls won't satisfy real-world audits or incident response. These aren't checkboxes at the end of delivery. They are design decisions from the first service boundary.
Interoperability is a product requirement
Enterprise-grade telemedicine platforms should use API-based modules and adhere to HL7 FHIR for clinical data exchange and DICOM for imaging, with a dedicated interoperability platform that can translate between formats rather than relying on proprietary interfaces (enterprise telemedicine architecture).
That recommendation sounds obvious until teams face a deadline. Then they hardcode one EHR workflow, map one lab feed in a custom way, and postpone standardization. The platform ships faster, but every new integration becomes a special project. Product velocity slows, onboarding costs rise, and data quality disputes multiply.
A better pattern looks like this:
-
Canonical data contracts: Normalize internal representations even if upstream systems vary.
-
Translation at the edge: Use interface engines or interoperability services to absorb external variance.
-
Versioned APIs: Don't let clinical workflow changes break downstream consumers.
-
Explicit ownership: Somebody has to own terminology mapping, payload quality, and schema evolution.
Security controls have to survive real operations
Healthcare systems don't fail security reviews because they forgot the word encryption. They fail because controls don't hold under support workflows, exceptions, and third-party dependencies.
That means designing for least privilege, auditable access, data segregation, consent-aware retrieval, and retention controls that match operational reality. It also means testing before an incident forces you to. A useful operational reference for securing patient data with pentesting can help teams pressure-test assumptions around exposed attack surfaces in HIPAA-relevant environments.
As we explored in our guide to HIPAA-compliant software development, strong compliance posture usually comes from mundane engineering discipline: clear service boundaries, complete logging, predictable access rules, and fewer undocumented exceptions. The teams that struggle most are usually the ones carrying years of ad hoc integration decisions.
Advanced Capabilities with AI Data and Edge Computing
Once the foundations are solid, differentiation comes from how well the platform interprets data and how reliably it responds under clinical pressure.
AI has a real role in virtual care infrastructure, but only where the workflow, signal quality, and accountability are clear. The useful applications are familiar: risk stratification, triage support, prioritization queues, anomaly detection from remote monitoring streams, and motion-aware safety support in virtual inpatient settings. The mistake is treating AI as a feature layer sitting above fragmented operations. It only works when the data path is disciplined.
Start with data flow, not model selection
Continuous physiologic data from wearables has to be ingested, normalized, and routed to the right care team in a clinically sensible way. If your pipeline accepts every signal but can't classify urgency, suppress noise, or connect events to the right protocol, you haven't created intelligence. You've created clinician burden.
A practical pattern is to split the pipeline into four parts:
-
Capture and normalization so different devices can be translated into a consistent internal model.
-
Rules and model services that classify urgency and surface exceptions.
-
Workflow routing that sends alerts to the right queue, role, or escalation path.
-
Feedback loops so false positives and triage misses improve the system over time.
AI development services and enterprise AI solutions become relevant, but only when they're tied to operational pathways clinicians will use.
Edge matters when seconds matter
For safety-critical virtual care, infrastructure guidance points to 99.999% high availability uptime, dedicated network segments for telehealth traffic, peer-to-peer protocols such as WebRTC to reduce latency-heavy VPN dependency, and edge computing to process clinical data locally instead of waiting for cloud roundtrips (digital hospital connectivity guidance).
That's not about architectural fashion. It's about choosing where computation happens.
Use cloud-heavy patterns when workloads are asynchronous, analytical, or batch-oriented. Use edge patterns when the application can't tolerate network jitter, dead zones, or delayed event handling. Virtual ICU, telesitting, and device-dense care environments push teams toward local processing, stronger wireless design, and direct media paths.
The cleanest AI demo often fails first in production because the network path is less reliable than the model assumptions.
Security still has to keep pace with those deployments. Teams evaluating distributed operations often benefit from broader operational guidance on healthcare IT security and compliance, especially when edge devices, care-site networking, and centralized oversight intersect. For a deeper architecture view, see our guide on mastering healthcare edge computing.
A Phased Implementation and Migration Roadmap
Replatforming virtual care infrastructure in one motion is how teams create outages, clinician frustration, and budget overruns. The safer approach is phased replacement with explicit handoff points.
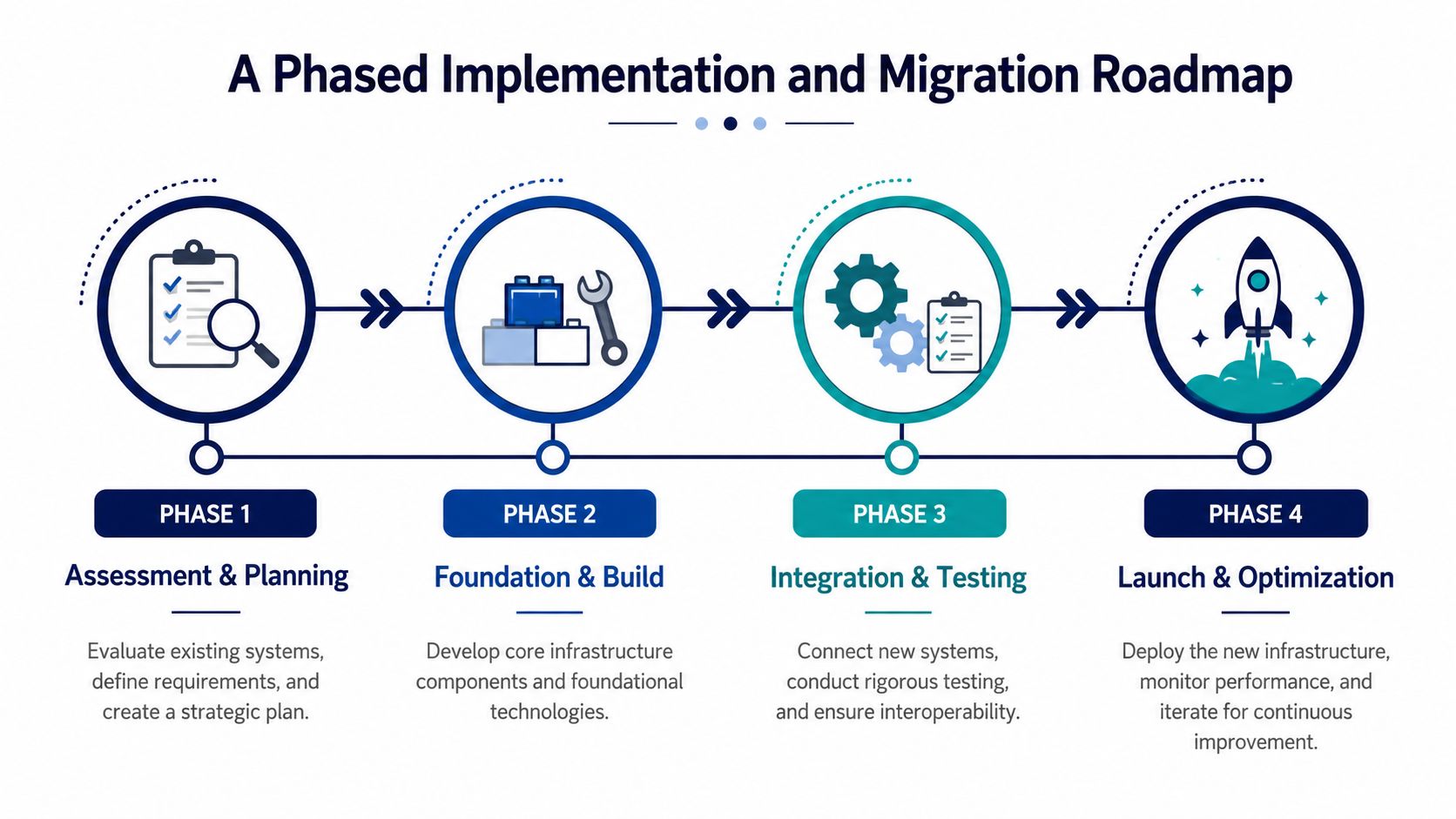
Phase 1: Assessment and planning
Start with system inventory, not aspiration. Map the actual patient, provider, support, billing, and integration flows. Most organizations discover they're running more manual exception handling than leadership realizes.
Key outputs in this phase:
-
Workflow maps: Where care starts, where it stalls, and where staff intervene manually
-
System boundaries: Which tools own identity, scheduling, charting, communication, billing, and reporting
-
Risk register: Fragile integrations, unsupported components, data duplication, and compliance gaps
-
Business priorities: Access growth, clinician efficiency, care continuity, payer readiness, or service-line expansion
This is also where team structure matters. Your software development service models should match the risk profile of the program. A platform modernization with live clinical workflows needs tighter product, engineering, QA, security, and integration coordination than a greenfield proof of concept.
Phase 2: Foundation and build
Build the shared services first. Identity, permissions, audit trails, encounter orchestration, communication abstraction, and interoperability services should be in place before you start polishing edge workflows.
If you're building a product business around care delivery, treat the platform as SaaS product development, not as a series of client-specific feature requests. The more bespoke branching you allow early, the harder it becomes to maintain compliance and uptime across deployments.
One implementation option in this stage is to engage a delivery team that already works across compliant healthcare builds, integrations, cloud services, and AI-assisted engineering. Bridge Global offers custom software development for that kind of cross-functional build, which is relevant when product and engineering leaders need one team spanning platform architecture, integration, and modernization work.
Phase 3: Migration and integration
Legacy retirement should happen by capability slice, not by system name. Move one flow at a time. Scheduling. Encounter launch. Documentation sync. Billing outputs. Device data. Language access. Support tooling.
A practical migration sequence usually includes:
-
Dual-run periods for critical workflows where old and new outputs can be compared.
-
Interface shims so dependent systems don't all need to change at once.
-
Targeted clinician pilots with support staff embedded in the rollout.
-
Rollback criteria defined before go-live, not during the incident call.
Migrations fail when teams confuse technical cutover with workflow adoption.
Phase 4: Launch and optimization
After launch, the backlog should shift from build requests to operational tuning. That means queue design, alert thresholds, patient completion rates, interpreter workflow, support content, and reimbursement edge cases.
If AI is on the roadmap, don't treat it as a separate innovation track. Tie it to the same governance process and use-case selection logic as the rest of the platform. A formal AI implementation roadmap helps teams avoid bolting predictive features onto unstable data paths.
Always check existing blog URLs before publishing new rollout documentation or technical notes, and use unique, descriptive slugs so migration knowledge stays searchable instead of colliding with earlier content.
Measuring Success KPIs and Commercial Considerations
The wrong KPI set makes a weak platform look healthy. If you only track visit volume, you won't see language access delays, clinician burden, or billing leakage until they become expensive.
A stronger measurement model combines operational, clinical, and commercial views. For inpatient and hybrid virtual care, effective strategies should be measured using the percentage of encounters using language access services, interpreter wait times, HCAHPS scores, average length of stay, and readmission rates, aligned to the four Cs of Consultation, Communication, Connection, and Control (inpatient virtual care strategy metrics).
The KPI set that actually helps operators
| Category | KPI | Description |
|---|---|---|
| Operational | Platform uptime | Indicates whether care can be delivered consistently across patient and provider workflows |
| Operational | Encounter completion rate | Shows how often scheduled visits reach a successful clinical endpoint |
| Operational | Percentage of encounters using language access services | Measures whether the platform is serving patients who need interpreter support |
| Operational | Average wait time for an interpreter | Exposes friction in multilingual care delivery |
| Clinical | HCAHPS patient satisfaction scores | Tracks patient perception before and after implementation |
| Clinical | Average length of stay | Helps evaluate whether virtual workflows support faster, safer throughput |
| Clinical | Readmission rates | Surfaces whether post-discharge and ongoing virtual support are clinically effective |
| Commercial | Claims acceptance trends | Reflects how well revenue-cycle logic aligns with payer requirements |
| Commercial | Utilization by service line | Reveals whether infrastructure supports real adoption, not just technical availability |
| Commercial | Support burden per encounter | Connects user experience design to staffing cost and scalability |
Tie metrics to decisions, not dashboards
Operational teams need different views from product leaders and finance teams. Don’t put every metric in one executive dashboard and call it observability.
Use KPI ownership deliberately:
-
Operations leaders need queue times, handoff failures, no-show recovery, and interpreter access.
-
Clinical leaders need quality and outcome measures tied to workflow changes.
-
Finance and product teams need utilization, reimbursement integrity, and support cost signals.
If your metrics don’t tell you where to invest next, they’re reporting artifacts, not management tools. That’s also why reviewing real client cases can be useful. Mature programs usually show clear alignment between platform architecture, workflow metrics, and business decisions.
Building for Equity and Trust, Not Just Technology
A virtual care platform can be technically excellent and still fail the populations that need it most.
Video-first design often reflects the assumptions of product teams with strong devices, stable broadband, high digital confidence, and quiet places to talk. Many patients don’t have those conditions. Research has shown that virtual care has widened disparities for low-income, Black, Hispanic, and older adult populations lacking video-capable devices or reliable broadband, and it recommends reimbursement parity for telephone visits plus low-bandwidth, audio-first modalities as core features (barriers to virtual care access).
Equity belongs in the architecture
That has direct infrastructure implications.
-
Audio-first pathways: Phone-based encounters can’t be treated as fallback hacks. They need scheduling, consent, documentation, and billing paths that are fully supported.
-
Low-bandwidth resilience: Connection downgrade logic, asynchronous follow-up, and lightweight interfaces matter in real-world access environments.
-
Multilingual access: Interpreter support and patient-facing content should be integrated into workflows, not pushed into call-center workarounds.
-
Simple patient support: Written instructions in plain steps and accessible support channels reduce drop-off long before clinical quality becomes the issue.
Another barrier gets less attention than connectivity: trust. A scoping review of virtual clinics in underserved regions highlights workforce resistance, privacy and data security concerns, targeted workforce training, patient technical support, and multilingual, patient-friendly design as major factors in adoption (review of virtual clinics in underserved regions).
Trust has to be designed, not assumed
Patients don’t separate technical reliability from institutional trust. If onboarding is confusing, if language support is delayed, if privacy expectations are unclear, or if the app fails during a sensitive visit, confidence drops quickly.
That’s why digital literacy belongs in infrastructure planning. So does workforce readiness. A clinician who doesn’t trust the routing logic or a patient who doesn’t understand the join flow can both break the service, even when the software is functioning exactly as designed.
If a patient can only access your platform under ideal technical conditions, your infrastructure strategy is incomplete.
The most durable virtual care systems don’t just connect people. They accommodate reality.
Frequently Asked Questions
What’s the biggest architectural mistake in virtual care infrastructure?
Coupling everything to one communication vendor is a common one. If your scheduling, encounter state, documentation flow, and provider controls depend directly on a single video SDK, replacing or upgrading that component becomes expensive and risky. Keep communication abstracted from the clinical core.
Should startups build around one flagship workflow first?
Yes, but the shared services still need discipline. You can start with one service line, one encounter type, or one patient segment. Don’t start with one-off logic everywhere. Identity, auditability, messaging, and interoperability should be reusable from the start.
When should teams introduce AI?
After the data path is reliable enough to support decisions. If device feeds are inconsistent, triage rules aren’t governed, or operations can’t review outputs, adding AI usually increases noise. Start with narrow use cases tied to an owned workflow.
Is audio-only really part of virtual care infrastructure?
Yes. If a significant share of your users can’t depend on video-capable devices or broadband, audio isn’t an edge case. It’s part of access architecture. Treating it as secondary usually creates inequity, workflow gaps, and reimbursement confusion.
What should leaders prioritize during migration?
Protect care continuity first. Run dual workflows where needed, define rollback rules before launch, and migrate by capability slice rather than trying to replace every legacy component in one cutover.
How do you know the platform is working commercially?
Look beyond raw visit counts. Track whether encounters complete successfully, whether claims move cleanly, whether support burden is dropping, and whether the platform expands access without creating hidden staffing cost or clinician friction.
If you’re planning a virtual care platform, modernizing a legacy telehealth stack, or defining an AI-enabled roadmap for connected care, Bridge Global can support the engineering, integration, and product architecture work behind compliant digital health systems.
About Preethi Saro Philip
Preethi Saro Philip is a Post Graduate Research Degree holder in Economics with more than 10 years of experience in writing, editing, research and teaching. She has an intense passion for content crafting and calls herself a ‘wordsmith’. She enjoys writing on wide-ranging topics including business, technology, health & lifestyle, education, environment etc.
View all posts by Preethi Saro Philip →