


A Guide to Hospital Management System Modernization
Most hospital leaders don't start thinking about hospital management system modernization because they want a new architecture diagram. They start because the current environment has become exhausting to run. Admissions rekey data into multiple systems. Finance depends on brittle interfaces. Clinical teams work around screens that don't reflect how care is delivered. Every upgrade window feels risky, and every integration request uncovers another hidden dependency.
That pressure is no longer isolated to a few early adopters. The global hospital management system software market was worth about USD 28 billion in 2023 and is projected to reach USD 59 billion by 2032, with a CAGR of roughly 8.5%, according to this market outlook on hospital management system software. That matters because modernization has moved out of the category of discretionary IT improvement. It now sits in the same conversation as resilience, compliance, operating margin, and care continuity.
A good modernization program doesn't begin with "replace everything." It begins with sequencing, risk control, and honest trade-offs. In cross-border environments, that also means understanding how connected data has to move outside the hospital's walls. For teams thinking through interoperability in regional care ecosystems, this perspective on integrating healthcare data in Canada is useful because it reflects the operational reality of coordination across providers, systems, and jurisdictions.
Leaders also need a clear picture of where automation creates value after the core platform is stabilized. This AI hospital automation whitepaper for healthcare operations is a relevant companion if you're already evaluating what should come after foundational modernization.
Why Modernize Your Hospital Management System Now
The immediate reason is usually friction. The deeper reason is risk concentration.
Legacy hospital platforms rarely fail in one dramatic moment. They fail by slowing everything around them. Integration work takes too long. Security patches become harder to apply. Reporting depends on manual reconciliation. Departments build local workarounds, then those workarounds become part of the unofficial operating model. Eventually, the hospital isn't running one system. It's running a fragile ecosystem of exceptions.
Operational pain turns into strategic exposure
When a hospital can't trust core workflows, the consequences go beyond IT. Revenue cycle teams spend more time correcting errors. Compliance teams struggle to prove lineage and control. Clinical staff lose confidence in screens that should support decisions but instead create noise.
That is why modernization should be treated as an operational redesign effort, not just a software refresh. The market direction supports that view. Hospitals aren't modernizing because it's fashionable. They're doing it because connected operations, cleaner data flows, and maintainable platforms now shape day-to-day performance.
Modernization succeeds when executives stop asking, "What system should we buy?" and start asking, "Which risks are we carrying today because our core systems can't evolve safely?"
Why waiting gets more expensive
Hospitals can delay visible transformation, but they can't pause system aging. Skills for older stacks become harder to source. Point integrations multiply. Audit and security obligations don't get simpler. Meanwhile, clinical and administrative teams still need better workflows now, not after a multi-year replacement gamble.
Three patterns usually signal that action can't wait:
-
Integration bottlenecks are affecting care and operations: New partner connections, patient services, or analytics initiatives stall because existing systems can't expose data cleanly.
-
Supportability is deteriorating: The hospital depends on a small group of people who understand brittle jobs, undocumented interfaces, or legacy databases.
-
Leadership lacks visibility into impact: Everyone knows the environment is painful, but no one has translated that pain into business risk, cost, and sequencing decisions.
Hospital management system modernization works best when those signals are treated as portfolio issues. That means ranking what threatens continuity first, protecting what must keep running, and building the future state in controlled phases.
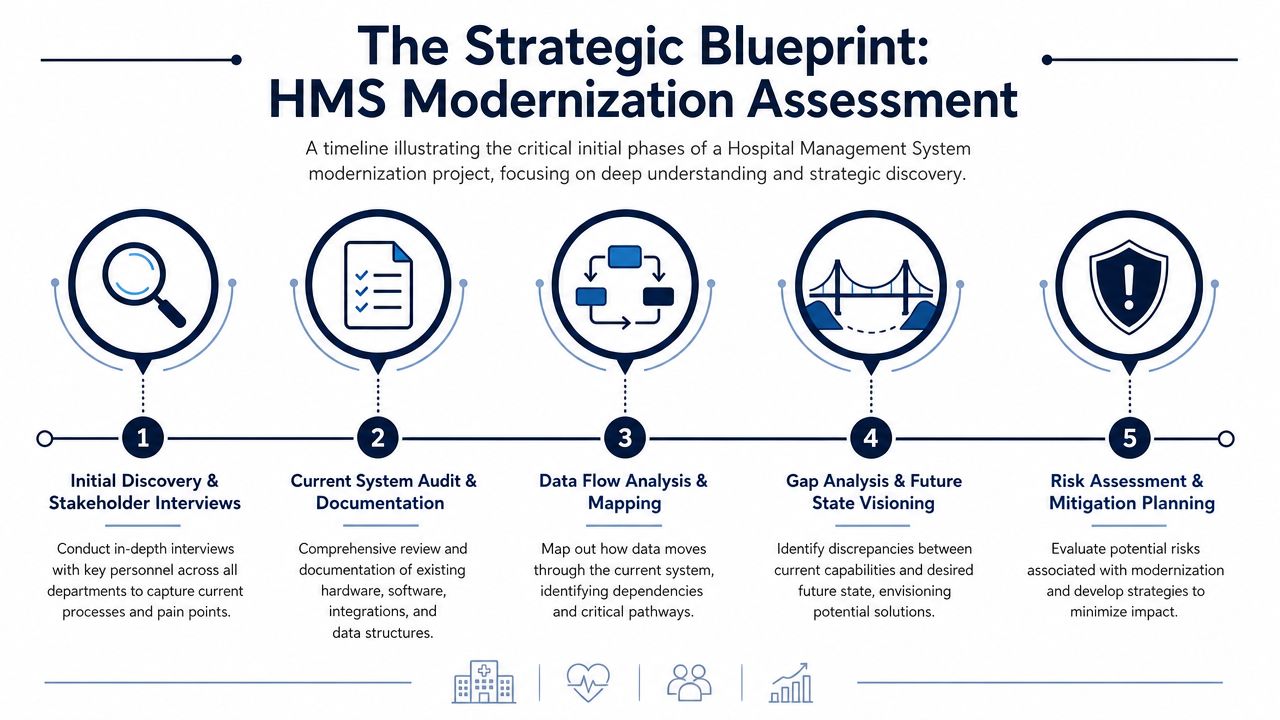
The Strategic Blueprint Assessment and Discovery
Most failed modernization programs fail before any migration starts. They fail during framing. Teams jump from dissatisfaction to solution selection without building a usable map of what exists, what matters, and what can break.
A proper assessment phase is less glamorous than architecture workshops, but it's where the project becomes real.
A 2021 HIMSS survey found that about 70% of U.S. healthcare organizations still relied on outdated legacy software, and a phased modernization approach focused on high-risk backend systems can yield a 25%–40% reduction in IT operational costs over three years, as summarized in this review of healthcare data management and predictive analytics. That combination explains why assessment has to focus on business-critical backend risk, not just visible user-facing complaints.
Start with business capability mapping
An application inventory alone isn't enough. You need to know which systems support which hospital capabilities, and where those capabilities cross departments.
For example, patient registration may involve the front desk, identity management, payer validation, clinical scheduling, document capture, billing, and downstream reporting. If you only catalog software names, you miss how a change in one place cascades elsewhere.
The first pass should answer questions like these:
-
Which applications support core capabilities?
Admissions, pharmacy, lab, radiology, claims, bed management, asset tracking, procurement, and reporting all need clear ownership.
-
Which interfaces are critical for daily continuity?
HL7 feeds, batch jobs, message brokers, flat-file exchanges, API calls, and manual exports all belong on the map.
-
Which systems create disproportionate drag?
Not necessarily the oldest ones. Usually, the ones with high dependency counts, poor documentation, or repeated incident patterns.
This stage often uncovers something executives haven't seen clearly. The most painful systems are not always the most visible ones.
Quantify the cost of doing nothing
Modernization proposals lose momentum when they sound like a technical preference. They gain traction when they show operational exposure in terms that leadership already understands.
Build dashboards that translate technical debt into business language:
| Focus area | What to measure qualitatively |
|---|---|
| Revenue risk | Claim delays, reconciliation effort, rework caused by broken handoffs |
| Compliance risk | Audit gaps, weak traceability, inconsistent access control, reporting fragility |
| Operational drag | Manual entry, repeated workarounds, dependency on specific individuals |
| Service continuity | Outage sensitivity, recovery complexity, integration brittleness |
The point isn't to produce false precision. The point is to stop discussing modernization as a generic platform upgrade.
Practical rule: If your executive briefing starts with technologies instead of risks, costs, and service continuity, you haven't finished discovery.
Build governance before tool selection
Neutral guidance on healthcare IT modernization recommends a staged process: identify pain points, quantify impact, brief executives, form an IT strategy committee, decide what can be handled internally, bring in vendors where needed, prototype options, then prioritize deployment. That sequence appears in this guidance on IT modernization in the healthcare industry.
That's also where a strong custom healthcare software development effort begins. Not with code, but with a governance model that can make trade-offs deliberately.
A practical discovery structure usually includes:
-
Executive sponsor group: Owns priorities, escalation paths, and funding decisions.
-
Clinical and operational stakeholders: Validate workflow reality and identify essential continuity requirements.
-
Architecture and security leads: Map dependency, supportability, and control gaps.
-
Program management office: Maintains scope discipline and sequencing.
Prioritize by risk and dependence, not age
Some old systems can stay stable for a while with API wrapping or infrastructure updates. Some newer systems deserve attention first because they sit on fragile data flows or support high-criticality services. Discovery should produce a modernization queue, not a wish list.
That queue typically separates systems into categories such as retain, encapsulate, rehost, re-architect, replace, or retire. The right answer depends on supportability, integration load, downtime tolerance, regulatory impact, and how central the system is to future workflows.
If discovery is done well, the hospital ends this phase with something much more valuable than an inventory. It has a modernization thesis.
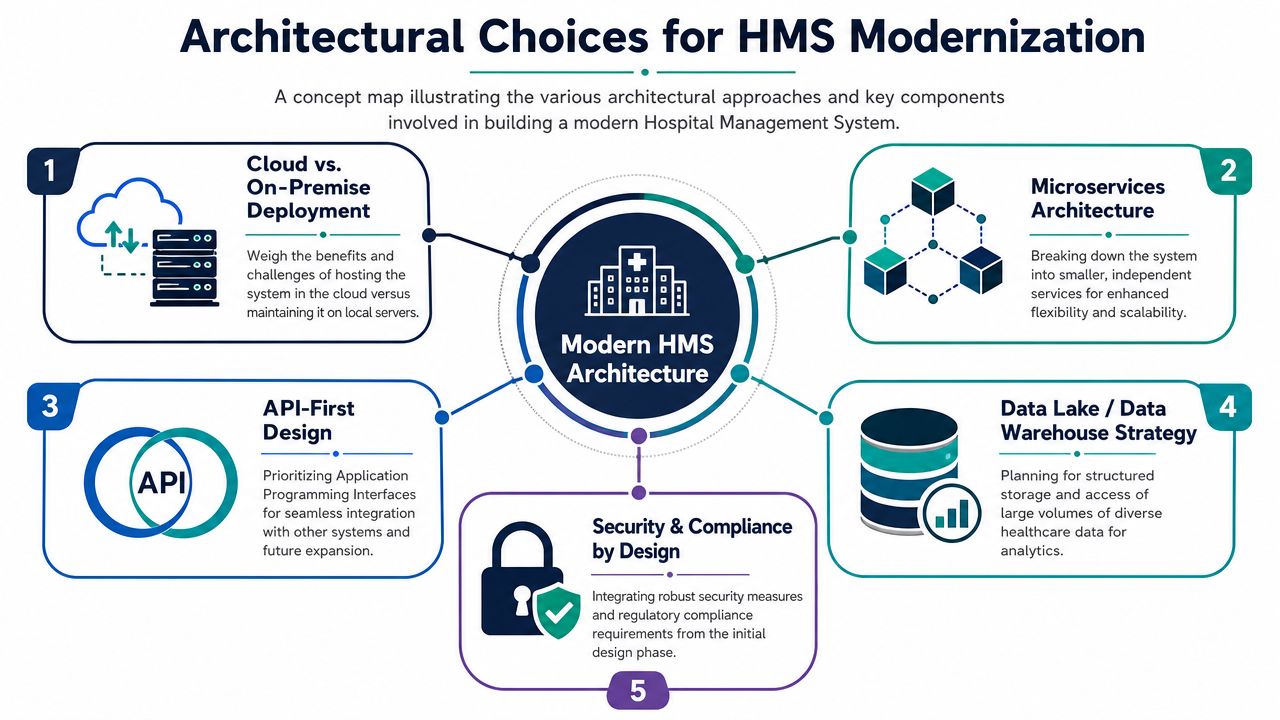
Choosing Your Modernization Architecture
Architecture decisions in healthcare aren't abstract engineering preferences. They determine how safely a hospital can evolve, how easily partners can connect, and how expensive future change becomes.
The biggest architectural mistake is building a newer version of the same isolation problem.
A 2026 review of healthcare data modernization identified persistent barriers in integration and interoperability, along with governance, privacy, data quality, and workforce capability. It also noted that projects often fail by replacing one silo with another unless they design around standards, governance, and real-time exchange from the start, as detailed in this review of healthcare data modernization barriers.
Cloud, on-prem, or hybrid
This decision is rarely ideological. It's operational.
A fully on-prem model may still make sense for specific workloads tied to local control, latency sensitivity, or organizational constraints. A cloud-first approach can improve scalability and reduce infrastructure burden, but only if identity, security controls, integration patterns, and cost governance are handled properly. Many hospitals land in a hybrid state because modernization has to coexist with clinical systems, device ecosystems, and partner networks that won't move at the same pace.
A simple comparison helps:
| Architecture path | Where it works well | Where it gets risky |
|---|---|---|
| On-prem | Tight local control, systems with fixed hosting constraints | Slower scaling, heavier infrastructure overhead |
| Public cloud | Elastic workloads, analytics, modern app services | Poor governance can create sprawl and compliance concerns |
| Private cloud | More controlled hosting model for sensitive workloads | Can recreate old complexity if poorly managed |
| Hybrid | Realistic transition path for complex hospitals | Integration and operating model can become messy fast |
The wrong choice isn't "cloud" or "on-prem." The wrong choice is selecting a hosting model without aligning it to workflow criticality, integration needs, and internal operating maturity.
Monolith, modular monolith, or microservices
Microservices are attractive because they allow separate deployment, clearer domain boundaries, and more targeted scaling. But hospitals shouldn't split everything into services on day one. If the team lacks observability, API governance, and disciplined domain ownership, microservices can produce distributed confusion.
In many hospital environments, a phased target state works better:
-
Keep stable core logic intact where change risk is high, and business rules are foundational.
-
Extract high-change domains first, such as scheduling, notifications, patient communication, or reporting services.
-
Expose capabilities through APIs before rewriting underlying logic.
-
Move toward service boundaries gradually as teams gain operational maturity.
A full rewrite remains the most time-consuming option. That's why selective re-architecture often beats wholesale replacement.
Hospitals don't need the trendiest architecture. They need an architecture that their teams can operate safely at 2 a.m. during a real incident.
Design interoperability from day one
Hospital management system modernization either provides a significant advantage or compounds future pain. Interoperability isn't solved by saying "we have APIs." The hard part is agreeing on what data means, how it is governed, and when it is exchanged.
For most hospitals, an interoperable architecture needs:
-
Standards-aware interfaces: HL7 and FHIR matter because external systems, labs, pharmacies, insurers, and public health interfaces rarely align by accident.
-
Canonical data models: Without shared internal meaning, every integration becomes custom translation work.
-
Real-time and event-aware patterns: Batch still has a place, but many workflows now need faster exchange and traceability.
-
Governance over endpoint growth: APIs without lifecycle control become another legacy layer.
Teams evaluating this area may also find this perspective on modern medicine's digital backbone useful because it frames infrastructure and integration as the underlying system that enables everything else.
Choose architecture based on future change
A hospital's architecture should answer one practical question. What kinds of change do we expect over the next few years?
If the organization needs faster partner integration, stronger analytics, and safer incremental delivery, then API-first design, modular service boundaries, and a clear data platform strategy usually make sense. If the immediate need is to stabilize hosting and reduce operational fragility, rehosting or selective refactoring may come first.
Architecture should never be chosen in isolation from the modernization sequence. It has to serve the rollout plan, the operating model, and the reality of constrained budgets.
Managing Critical Assets Data and Security
Many teams still treat data migration and security as downstream workstreams. In hospital environments, that's backwards. They are design constraints from day one.
If the data is dirty, poorly governed, or impossible to validate, the new platform inherits old risk. If security is bolted on after architecture decisions are made, the hospital pays for that compromise repeatedly.

Reviews of hospital information system implementation point to recurring failure modes such as poor data quality, lack of system integration, inadequate skills and training, insufficient financial support, and weak management/change control. The same review notes that success depends on investment in technology and user infrastructure, active data-quality control, and a strong safety culture with feedback loops, as described in this evidence review on hospital information system implementation success factors.
Treat migration as clinical and operational risk management
Data migration isn't only about moving tables from one system to another. It involves deciding what data remains authoritative, what gets archived, what must be transformed, and what cannot be trusted without remediation.
A practical migration plan usually includes these tracks:
-
Data profiling: Identify duplicates, missing fields, inconsistent coding, and values that won't fit the target model.
-
Data ownership: Assign business owners who can approve mapping rules and exception handling.
-
Validation design: Define how the hospital will compare source and target outputs before go-live.
-
Cutover planning: Decide which transitions can happen incrementally and which need coordinated windows.
Teams often underestimate the amount of historical data that no one uses, but everyone assumes must move. That assumption creates cost, delay, and validation burden.
Protect critical assets first
Hospitals don't modernize software in a vacuum. They run networks of applications, devices, support platforms, maintenance systems, and operational assets with unequal risk. Security and continuity planning should reflect that.
A useful prioritization lens looks like this:
| Asset type | Modernization concern | Priority question |
|---|---|---|
| Core clinical systems | Downtime and data integrity | What must never lose continuity? |
| Integration middleware | Hidden dependency concentration | What breaks if this layer stalls? |
| Identity and access services | Access control and auditability | Can users be governed consistently? |
| Departmental legacy apps | Shadow workflows and unsupported logic | Is this app critical or just familiar? |
That approach aligns with how risk should be managed in high-stakes environments. Protect the assets whose failure creates the widest operational blast radius.
Security architecture should follow patient risk, not just compliance checklists.
Build security into delivery, not after it
Hospitals need a security-by-design posture. That means decisions about authentication, authorization, encryption, audit logging, segmentation, monitoring, and recovery are embedded in architecture and release processes.
In practice, this includes:
-
Threat modeling early: Before development teams lock in trust boundaries and integration methods.
-
Role and access design: Based on real operational responsibilities, not generic user buckets.
-
Audit-ready logging: Events need to be attributable, searchable, and retained appropriately.
-
Continuous monitoring: Connected environments need visibility into anomalous behavior and integration failures.
-
Recovery testing: Backups matter, but tested recovery matters more.
This is also why hospitals often need disciplined support from teams experienced in secure custom software development and operational controls. For organizations strengthening the protection side of modernization, dedicated cybersecurity services are often part of the broader program, not a separate purchase later.
Don't ignore user infrastructure
Technical teams sometimes talk about security as if users are external to the system. In reality, users are part of the system. Weak workstation practices, poor training, workaround culture, and unclear escalation paths can undo strong technical controls.
A safer modernization program invests in training, incident feedback loops, clear reporting paths, and realistic workflow design. That doesn't slow delivery. It prevents avoidable failure.
Unlocking Intelligence with AI, ML, and BI
Once the hospital has a cleaner architecture, controlled data flows, and more reliable operational foundations, AI, ML, and BI stop being slideware. They become usable tools.
The important point is sequencing. Intelligence layers only create value when the underlying system produces trustworthy, timely, governed data.

BI usually creates the first visible wins
Before an organization deploys advanced models, it often gets immediate value from better visibility. Business intelligence dashboards can unify operational signals that were previously scattered across departmental tools, spreadsheets, and delayed reports.
In hospitals, that often means dashboards for:
-
Patient flow oversight: Bed availability, discharge bottlenecks, transfer status, and queue pressure.
-
Revenue cycle monitoring: Exceptions, denials' worklists, reconciliation delays, and aging process gaps.
-
Operational control rooms: Service desk trends, interface failures, backlog status, and cutover readiness during rollout.
These aren't glamorous use cases, but they matter. A modern hospital management system should allow leaders to see the operation they are running, not the one they assume they are running.
AI should start where decisions repeat
The best early AI use cases in healthcare operations are usually bounded, repetitive, and measurable. Administrative automation often qualifies before complex clinical decision support does.
Examples include:
-
routing and classifying inbound operational requests
-
summarizing support tickets or workflow exceptions
-
surfacing missing documentation patterns
-
prioritizing queues for finance or back-office review
-
detecting process anomalies across transactions and events
That doesn't mean AI belongs only in administration. It means hospitals should start where governance is simpler, explainability is manageable, and adoption barriers are lower.
A good AI implementation roadmap usually ties use cases to data readiness, workflow fit, review requirements, and operational ownership. The technical build then follows the business case.
The fastest way to discredit AI in a hospital is to deploy it on top of poor process design and unreliable data.
ML needs operational grounding
Machine learning can support forecasting, anomaly detection, and pattern recognition, but it can't compensate for fragmented source systems and undefined ownership. Teams need clear feature sources, validation methods, human review points, and drift monitoring.
That is why organizations should treat ML as part of platform modernization, not a separate innovation lab exercise. The delivery model has to connect data engineering, application engineering, domain experts, and operations.
Hospitals planning this layer often need access to specialized AI development services, particularly when they are moving from reporting to model-enabled workflows. The same applies to larger enterprise AI solutions that span multiple business functions rather than a single proof of concept.
The modern HMS becomes a platform
This is the larger shift. A modernized hospital management system isn't just a replacement for legacy administration software. It becomes a platform for controlled experimentation.
That platform can support:
| Capability | What it enables |
|---|---|
| Unified data access | Better dashboards, analytics, and cross-functional reporting |
| Event-driven workflows | Faster response to operational changes |
| Service-based architecture | Easier insertion of automation into specific processes |
| Governed APIs | Safer integration with internal tools and partner systems |
For product-minded healthtech teams, the same foundations also matter in adjacent platform work such as SaaS product development. The difference is that in hospitals, every intelligent feature has to coexist with auditability, workflow stability, and user trust.
From Plan to Practice Rollout and Partner Models
Rollout is where strategy meets institutional reality. This is the part that exposes whether the modernization plan was built for a hospital or for a demo environment.
Most organizations don't struggle because they lack a target architecture. They struggle because they underestimate sequencing, training, partner fit, and internal capacity.
Big bang versus phased rollout
A big bang rollout looks efficient on paper. One date, one cutover, one transition story. In hospital environments, it often concentrates too much risk.
Phased rollout usually works better because it lets teams isolate dependencies, validate assumptions, and correct issues before they spread. But phased doesn't mean slow or indecisive. It means changes are grouped by operational logic.
A practical comparison:
| Rollout model | Strength | Main risk |
|---|---|---|
| Big bang | Fast transition to target state | Broad operational disruption if assumptions fail |
| Phased by function | Clear business alignment | Cross-functional dependencies can linger |
| Phased by site or department | Easier local support and training | Temporary process variation across the organization |
| Parallel run for selected flows | Higher confidence during transition | Extra workload and reconciliation effort |
The right choice depends on workflow criticality, local support maturity, cutover tolerance, and how much coexistence the hospital can safely manage.
Modernize the riskiest assets first
Good guidance on legacy modernization in healthcare emphasizes asset discovery and risk prioritization, arguing that high-criticality assets with maintenance gaps should be modernized first, rather than following a blanket rip-and-replace approach. This perspective appears in this guidance on modernizing legacy systems in healthcare.
That is the right instinct. Not every old application deserves immediate investment, and not every newer one is safe to leave untouched.
A strong rollout queue usually gives priority to assets that are:
-
tightly connected to multiple workflows
-
hard to recover when they fail
-
weakly maintained or poorly documented
-
limiting security controls or auditability
-
blocking future integration work
Choosing a partner and delivery models
Hospitals have several delivery options. Internal teams can own strategy and vendor management while external specialists accelerate engineering. Some organizations bring in a focused architecture and integration partner. Others need a broader build model spanning discovery, modernization, data, QA, and rollout support.
What matters isn't just technical capability. It's healthcare operating awareness.
When evaluating delivery models, ask:
-
Can the partner work inside regulated delivery constraints?
-
Do they understand phased coexistence, not just greenfield delivery?
-
Can they support integration-heavy programs with multiple stakeholders?
-
Will they document decisions in a way that internal teams can sustain?
Those questions matter just as much as velocity. The same applies when reviewing software development service models for cost control, team structure, and long-term supportability.
Adoption is part of the rollout plan
Hospitals don't adopt new systems just because the functionality is available. They adopt when workflows make sense, training is role-specific, and support channels are responsive.
Useful rollout practices include:
-
Super-user networks: Local champions who can translate the change into department-specific practice.
-
Hypercare periods: Short-term intensified support after go-live.
-
Issue triage discipline: A visible system for distinguishing defects, training needs, and change requests.
-
Feedback loops: Staff need to see that reported friction leads to action.
If you're assessing execution maturity, relevant client cases can help show how different delivery approaches play out in real settings. The lesson is usually the same. Strong programs treat rollout as organizational change with technical components, not the other way around.
Measuring Success and Demonstrating ROI
If the business case only appears at funding time, the modernization program will struggle later. Success has to be measured against the same operational problems that justified the work.
That means tracking business-facing outcomes, not only technical completion.
Measure what leadership actually cares about
A useful measurement model covers four dimensions:
-
Operational continuity: Are critical workflows more stable and easier to support?
-
Process performance: Are teams spending less time on manual correction, duplicate entry, and workaround-heavy tasks?
-
Risk reduction: Has the hospital improved visibility, control, and recoverability in the areas that mattered most?
-
Platform readiness: Can the organization now support better integrations, reporting, and incremental change?
Some of these indicators are numeric inside the hospital, but they should come from the organization's own baseline and governance model, not from generic benchmarks pasted into a board deck.
Tie outcomes back to the original modernization thesis
The strongest ROI story isn't "we finished the project." It's "we reduced the specific operational burdens we identified in discovery."
A simple executive scorecard often works better than a sprawling transformation report:
| Original problem | Evidence of improvement |
|---|---|
| Fragile integration landscape | Fewer critical failures, clearer ownership, faster issue isolation |
| Manual operational workarounds | Reduced reliance on shadow processes and duplicate entry |
| Weak visibility | Better reporting and decision support for operational leaders |
| Hard-to-change core systems | Safer release patterns and clearer roadmap for next-stage improvements |
If the board can’t see how modernization improved resilience, efficiency, and control, the program will be remembered as a technology expense.
ROI in hospital management system modernization is cumulative. The first gains often come from stability, supportability, and reduced friction. Larger returns come later, when the hospital can add analytics, automation, and new services on top of a system that no longer resists change.
Frequently Asked Questions
How do hospitals decide what to modernize first?
Start with dependency mapping and risk ranking. The first candidates aren’t always the oldest applications. They are the ones whose failure creates the biggest operational, security, or compliance exposure. Systems with high criticality, poor maintainability, and many downstream dependencies usually move up the queue.
Is a full replacement ever the right choice?
Yes, but less often than teams first assume. A full rewrite or replacement can be justified when the existing platform is no longer supportable, blocks essential workflows, and can’t be safely extended. It remains the heaviest option, so the decision should come after discovery, architecture review, and a realistic rollout plan.
How do hospitals modernize without disrupting care delivery?
By sequencing around continuity. That usually means phased rollout, temporary coexistence where necessary, strong cutover planning, validation of high-risk data flows, and department-specific training. Hospitals that treat modernization like an all-at-once technology switch tend to create avoidable operational stress.
What usually goes wrong in modernization programs?
Common problems include weak data quality, poor integration planning, unclear governance, underfunded change management, and limited user training. Another frequent mistake is solving visible interface problems while leaving the hardest backend risks untouched.
Where should AI fit into the roadmap?
After the hospital has established cleaner data flows, clearer ownership, and a stable operating platform. AI and ML create more value when they support defined workflows, repeatable decisions, and governed data. If the foundation is weak, AI tends to expose process problems rather than solve them.
Should a hospital use one partner or several specialists?
It depends on internal maturity. Some hospitals benefit from a single accountable partner with a broad delivery scope. Others prefer a lead architecture partner plus targeted specialists for security, integrations, or analytics. The key is clear governance, decision ownership, and documentation that internal teams can sustain after rollout.
Hospitals don’t need another modernization pitch. They need a plan that respects continuity, budget pressure, interoperability, and the nature of regulated delivery. If you’re looking for a healthtech software development partner with experience in AI-enabled engineering, healthcare platforms, and complex modernization paths, Bridge Global is worth considering. Their work spans compliant healthcare solutions, secure delivery, integration-heavy systems, and scalable product engineering for organizations that need to modernize without losing control.
About Preethi Saro Philip
Preethi Saro Philip is a Post Graduate Research Degree holder in Economics with more than 10 years of experience in writing, editing, research and teaching. She has an intense passion for content crafting and calls herself a ‘wordsmith’. She enjoys writing on wide-ranging topics including business, technology, health & lifestyle, education, environment etc.
View all posts by Preethi Saro Philip →