


A Guide to Mastering Healthcare Platform Scalability
Your team probably knows this moment.
The platform is gaining traction. A pilot turns into a multi-site rollout. More clinicians log in at the same time, device feeds arrive in bursts, and a workflow that felt smooth in staging starts lagging in production. In healthcare, that isn't just a performance problem. It can turn into delayed decisions, broken trust, audit exposure, and real patient risk.
Healthcare platform scalability isn't about bragging rights on throughput. It's about keeping systems safe, compliant, interoperable, and dependable while your product, customer base, and data footprint expand. If you're choosing a healthtech software development partner, this is the lens that matters.
As we explored in our guide to platform engineering, healthtech teams don't usually fail because they lacked features. They fail because architecture, operations, and governance were treated as separate tracks until growth forced them together.
Why Scalability is a Mission-Critical Imperative
Most healthcare platforms don't break when they're ignored. They break when they succeed.
A provider signs a larger contract. A payer asks for more integrations. A remote monitoring workflow adds new cohorts. Suddenly the same platform has to support more concurrent sessions, more message traffic, more audit events, more support tickets, and more clinical dependency. If the core architecture was assembled layer by layer, every new demand creates friction in three places at once: the user experience, the compliance posture, and the operations model.
Healthcare leaders should take that pattern seriously. Industry analyses indicate that up to 70 to 85% of digital transformation initiatives in healthcare underperform or fail to scale effectively, largely because platforms are retrofitted layer by layer until scalability becomes prohibitively expensive.
Growth pressure changes the architecture question
Early on, teams can survive with manual workarounds. Engineers watch logs directly. Support teams escalate exceptions by chat. Product teams postpone deeper redesigns because shipping the next feature feels more urgent.
That stops working once the platform becomes operational infrastructure for care delivery.
Three shifts happen at that point:
Performance becomes a safety concern: Slow response times in a clinical workflow aren't the same as a slow ecommerce checkout.
Availability becomes contractual: Enterprise buyers expect resilience, incident response, and traceability.
Compliance becomes distributed: PHI doesn't stay inside one database and one app boundary once integrations, analytics, and AI services expand.
Practical rule: If a service outage can delay care coordination, consent validation, or clinical documentation, scalability is already a board-level issue.
Market growth will punish weak foundations
The demand side is moving quickly. The global market for healthcare data platforms is projected to reach $4.5 billion by 2033 and $5.4 billion by 2034, growing at a 20.3% CAGR, according to this healthcare data platform market projection. The same source notes that cloud-based deployment holds a 58.6% share in related healthcare digital experience platforms.
That matters because market growth doesn't reward fragile systems. It rewards teams that can onboard new organizations, connect new data sources, and support more workflows without rebuilding the stack every quarter.
Scalability in healthtech is strategic for another reason. Buyers increasingly expect one platform to support scheduling, clinical data exchange, patient engagement, analytics, and AI-enabled workflows together. If your architecture can't absorb that expansion, a competitor with a cleaner foundation will.
What works and what doesn't
What works is designing for operational load, integration complexity, and auditability from day one, even if the first release remains modest.
What doesn't is assuming you'll “split the monolith later,” “add compliance controls later,” or “standardize the data model later.” Later is where healthcare software gets expensive.
The Unique Challenges of Scaling in Healthcare
Generic SaaS advice falls short in healthcare because the hard part isn't only traffic. The hard part is scaling under clinical, regulatory, and interoperability constraints that don't bend when your roadmap gets aggressive.
Interoperability is the real bottleneck
A platform can run on modern cloud infrastructure and still fail at scale if data exchange is brittle. That's common when teams build fast with custom payloads, one-off mappings, and direct point-to-point interfaces that no one wants to touch after launch.
The core issue is simple. Scalability without interoperability is a false economy. If HL7 and FHIR workflows fail under growth, the platform doesn't scale across organizations, geographies, or adjacent product lines. It just accumulates technical debt faster.
In practice, many healthcare integration efforts often demonstrate their vulnerability in such situations:
Legacy EHR realities: Hospitals rarely expose clean, uniform interfaces.
Workflow mismatch: Two systems may both support FHIR, yet still model encounters, consents, or observations differently.
Operational drift: Interface rules that worked for one site become unmanageable across many.
For teams pursuing custom healthcare software development, interoperability-first design is more important than abstract cloud purity.
Equity doesn't scale automatically
Another problem is usually missed until late. Teams often ask how to scale infrastructure while overlooking who the platform serves well and who it leaves behind.
The most frequently asked but poorly answered question is, “How do we scale while maintaining true health equity?” Existing content often treats scalability as a technical metric while ignoring the equity paradox, as AI tools often do not work equally effectively for all patient interactions regardless of language, according to this PMC discussion of equity in health AI deployment.
That should change how CTOs define readiness. A system isn't scalable in any meaningful healthcare sense if it performs cleanly in one language, one literacy level, or one care setting while degrading for underserved populations.
Scale that widens disparities is not mature scale. It's operational expansion with ethical debt.
Compliance pressure multiplies with every new service
HIPAA and GDPR don't become easier when you add more APIs, more microservices, more vendors, and more analytics pipelines. They become harder because the number of trust boundaries grows.
The practical implications are familiar:
| Risk area | What changes at scale |
|---|---|
| Access control | More user roles, partner users, service accounts, and edge cases |
| Auditability | More events to capture, correlate, retain, and review |
| Consent handling | More downstream systems need policy-aware access decisions |
| Incident response | More components increase the blast radius of misconfiguration |
This is why healthcare teams can't treat compliance as a documentation exercise. It has to be embedded in architecture, delivery workflows, and production operations.
Downtime has a different meaning in healthcare
A consumer app can sometimes degrade gracefully and recover later. A health platform tied to patient communication, clinical review, care coordination, or documentation sits much closer to operational harm.
That changes design choices. You need explicit failure modes. You need dependency maps. You need a clear answer to a basic question: if one subsystem stalls, which clinical workflows must continue anyway?
Core Architectural Patterns for Scalable Health Platforms
Architecture decisions in healthtech should be made around isolation, interoperability, auditability, and failure containment. Raw developer preference isn't enough.
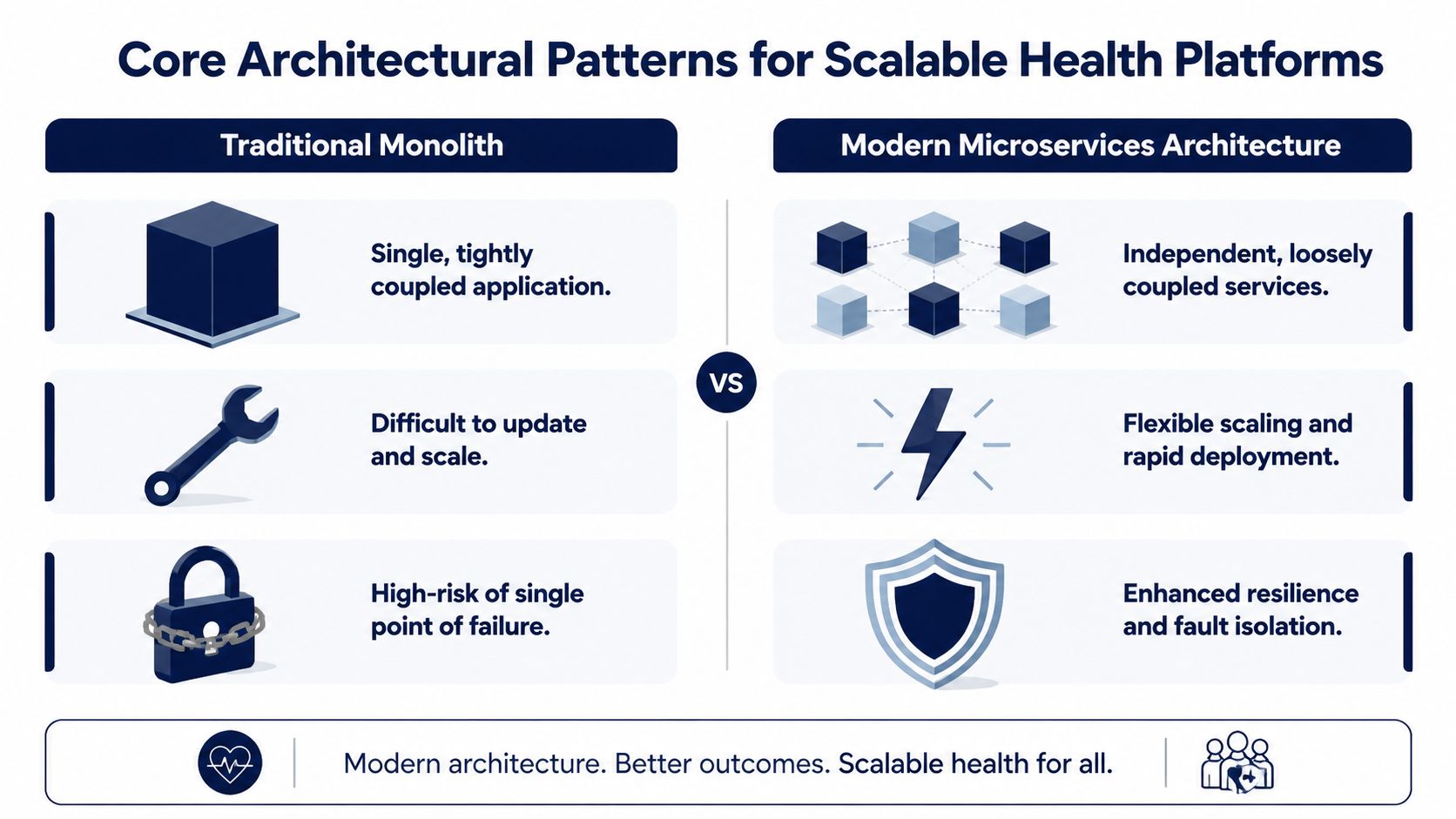
Start with modularity, not ideology
A monolith isn't automatically wrong. For a narrow product with a small team, a well-structured modular monolith can be a better first step than premature service sprawl. You get simpler deployment, fewer network boundaries, and less operational overhead.
The problem starts when teams confuse a monolith with a long-term scaling plan.
Once appointment scheduling, patient identity, messaging, billing, document ingestion, and analytics all sit in one codebase with one deployment rhythm, every release becomes harder to test, and every incident becomes harder to isolate. In healthcare, that raises both reliability and compliance risk.
Why microservices fit health platforms better over time
The advantage of microservices isn't fashion. It's control.
Scalable platforms rely on containerized integration services orchestrated via Kubernetes for horizontal scaling, microservices to allow independent scaling of high-load functions, and API Gateways as centralized entry points to streamline client-service communication, as described in Emorphis' overview of healthcare integration architecture.
That directly supports healthcare use cases:
Patient identity can scale independently from content management or scheduling.
Integration engines can absorb interface load without forcing the whole application to scale.
PHI-heavy services can be isolated with tighter controls and narrower blast radius.
Deployment risk drops because teams can roll out changes to one service without redeploying every capability.
If you're designing a platform API layer, the engineering patterns in this guide to healthcare platform API engineering are a useful companion.
Event-driven architecture solves a different problem
Microservices handle component independence. Event-driven architecture handles coordination under change.
This pattern works well when systems need to respond asynchronously to clinical and administrative events. A lab result arrives. A consent changes. A new device reading lands. A referral status updates. Not every action should happen inside a synchronous request chain.
Used correctly, event-driven design helps with resilience and decoupling. Used carelessly, it creates opaque flows that are hard to audit.
In healthcare, asynchronous doesn't mean ungoverned. Every event still needs lineage, ownership, and replay discipline.
Architectural Pattern Comparison for HealthTech
| Attribute | Monolith | Microservices | Event-Driven |
|---|---|---|---|
| Deployment model | Single deployable unit | Multiple independently deployable services | Services coordinated through events and messaging |
| Operational simplicity | Higher at the start | Lower at the start | Lower, especially without mature tooling |
| Independent scaling | Limited | Strong | Strong for bursty and asynchronous workloads |
| Fault isolation | Weak | Better | Better, if consumers are isolated well |
| Compliance boundary control | Harder as scope grows | Easier to isolate sensitive domains | Strong for decoupling, but governance must be explicit |
| Interoperability fit | Often becomes tangled | Good with API-first design | Good for notifications, synchronization, and workflow triggers |
| Debugging complexity | Lower initially | Higher | Highest without robust tracing |
| Best fit | Early, tightly scoped products | Expanding multi-domain platforms | Platforms with many cross-system workflows |
Security and resilience choices are architectural choices
Health platforms need more than scale-out patterns. They need defensive layers around those patterns. API gateways, reverse proxies, network segmentation, and workload-level identity all matter once partner systems, mobile clients, devices, and analytics tools connect to the same platform.
For a useful security perspective on where healthcare information systems stay exposed in practice, see Vulnsy's healthcare security insights.
Teams building custom software development programs or new SaaS product development initiatives should choose architecture based on operational maturity, not trend pressure. The right question isn't “Should we use microservices?” It's “Which boundaries need independent scale, stronger isolation, and safer releases right now?”
Cloud, DevOps, and Observability Strategies
A clean architecture on paper doesn't help much if deployments are fragile, environments drift, and no one can explain why latency spikes under load.

Cloud gives you elasticity, not discipline
AWS, Azure, and GCP can all support healthcare platform scalability. The provider matters less than the operating model you build on top of it.
Use cloud services where they reduce undifferentiated work. Managed databases, managed Kubernetes, object storage, secret management, and policy tooling usually make sense. But don't assume a cloud migration fixes poor service boundaries or weak release processes. It doesn't.
A practical cloud baseline includes:
Autoscaling where demand is variable: Integration services and API workloads often need this first.
Clear environment separation: Development shortcuts must never leak into production handling of PHI.
Backup and recovery design: Recovery isn't a compliance checkbox. It's a clinical continuity requirement.
The platform also needs measurable performance expectations. A unified health data platform demonstrated near real-time performance for approximately 1,500 users on a single CPU-based server, with end-to-end delays remaining below 10 minutes, according to this evaluation of a unified health data platform. The lesson isn't that one server is enough for every platform. The lesson is that efficient architecture matters before you throw more infrastructure at the problem.
DevOps is how you scale change safely
Most healthcare outages I've seen weren't caused by traffic alone. They were triggered by release friction, config drift, or unclear ownership during change.
A mature DevOps model reduces those failures. It doesn't just speed up delivery. It gives teams repeatability.
Use these controls as essential requirements:
CI with meaningful validation: Unit tests aren't enough. Add contract tests, security checks, and integration test coverage for FHIR and HL7 paths.
CD with approvals that fit risk: Low-risk UI changes and high-risk workflow changes shouldn't move through the same gate.
Infrastructure as code: Manual production setup creates invisible variance you will pay for later.
Teams evaluating software development service models should ask how release ownership, compliance evidence, and production support are handled, not just how quickly code is written.
Observability is the only way to run distributed healthcare systems
As systems decompose, troubleshooting gets harder. An API request may touch an identity service, a consent service, a FHIR repository, a notification worker, and an external EHR connector. Without end-to-end visibility, every incident turns into guesswork.
Your minimum observability stack should cover:
Metrics for latency, error rates, saturation, queue depth, and integration throughput
Structured logs with correlation identifiers
Distributed tracing across synchronous and asynchronous flows
As we explored in our guide to cloud infrastructure for healthcare systems, observability has to map to clinical operations, not just infrastructure health. A green dashboard doesn't mean the referral workflow completed, the consent was honored, or the discharge summary reached the right destination.
Scaling Data, Compliance, and AI Lifecycles
Data scale, compliance scale, and AI scale are usually discussed as separate topics. In production health systems, they're tightly connected. If you architect them separately, one will eventually break the others.

Data architecture has to absorb variety, not just volume
Healthcare platforms don't deal with one neat transactional dataset. They handle structured clinical records, claims-like data, device streams, documents, images, consent artifacts, and operational telemetry.
That creates two common mistakes. First, teams try to force everything into one transactional store. Second, they create disconnected specialty stores with weak governance between them.
A better pattern is a governed data architecture with clear responsibilities:
| Data concern | Practical scaling approach |
|---|---|
| Transactional workflows | Keep them in operational stores designed for consistency |
| Large files and imaging | Use object storage with metadata and lifecycle controls |
| Analytics and reporting | Move curated datasets into dedicated analytical layers |
| Cross-system sharing | Standardize exchange through FHIR-aligned APIs and canonical models |
Interoperability-first thinking proves its worth. The system should be able to ingest, normalize, route, and expose data without rewriting domain logic every time a new partner arrives.
Compliance controls must be operationalized
At small scale, teams can paper over weak governance with manual review. At platform scale, that fails quickly.
Compliance at scale means the platform should produce evidence continuously. Audit trails, access decisions, data lineage, retention handling, and consent-aware policy enforcement need to be built into the platform's operating model.
A few patterns consistently work:
Policy-based access control: RBAC alone usually becomes too coarse as organizations and user roles multiply.
Immutable audit event capture: You need a reliable account of who accessed what, when, and under which authority.
Service-to-service trust controls: Internal traffic still needs authentication, authorization, and logging.
Automated security validation: Especially in environments with many endpoints and dependencies.
For teams strengthening security validation in distributed environments, resources on automated pentest solutions for MSPs are useful because they show how continuous testing can fit into a broader operational security program.
AI raises the bar on data governance
Healthcare AI doesn't scale safely unless the underlying data contracts are stable and traceable. Training pipelines, feature generation, model deployment, and post-deployment monitoring all depend on disciplined data handling.
The commercial pressure is obvious. The global AI-driven digital healthcare market is projected to expand from $15.1 billion in 2022 to over $187.9 billion by 2030, driven by clinical efficacy and adapting regulatory frameworks, according to this PMC review of AI-driven digital healthcare.
That doesn't mean every platform should rush models into production. It means CTOs need to treat AI as a lifecycle with controls.
A model endpoint without monitoring, lineage, and rollback is just another unmanaged clinical dependency.
The practical checklist looks like this:
Training data governance: Know what data entered the pipeline and under what permissions.
Model serving boundaries: Deploy models as isolated services with explicit versioning.
Bias and drift monitoring: Especially important where language, population, or workflow differences affect output quality.
Human override paths. Clinicians need clear escalation and review options.
If you're shaping the delivery plan for AI development services or broader enterprise AI solutions, the architecture should connect AI operations with compliance and interoperability from the start.
As we explored in our guide to healthcare data pipeline architecture, the handoff between operational systems and analytical or AI pipelines is one of the most failure-prone seams in healthtech. It deserves first-class design attention.
A Practical Roadmap for Scaling Your Platform
A dramatic rebuild is often unnecessary. What's needed is a sequence of decisions that matches product maturity, customer complexity, and regulatory exposure.
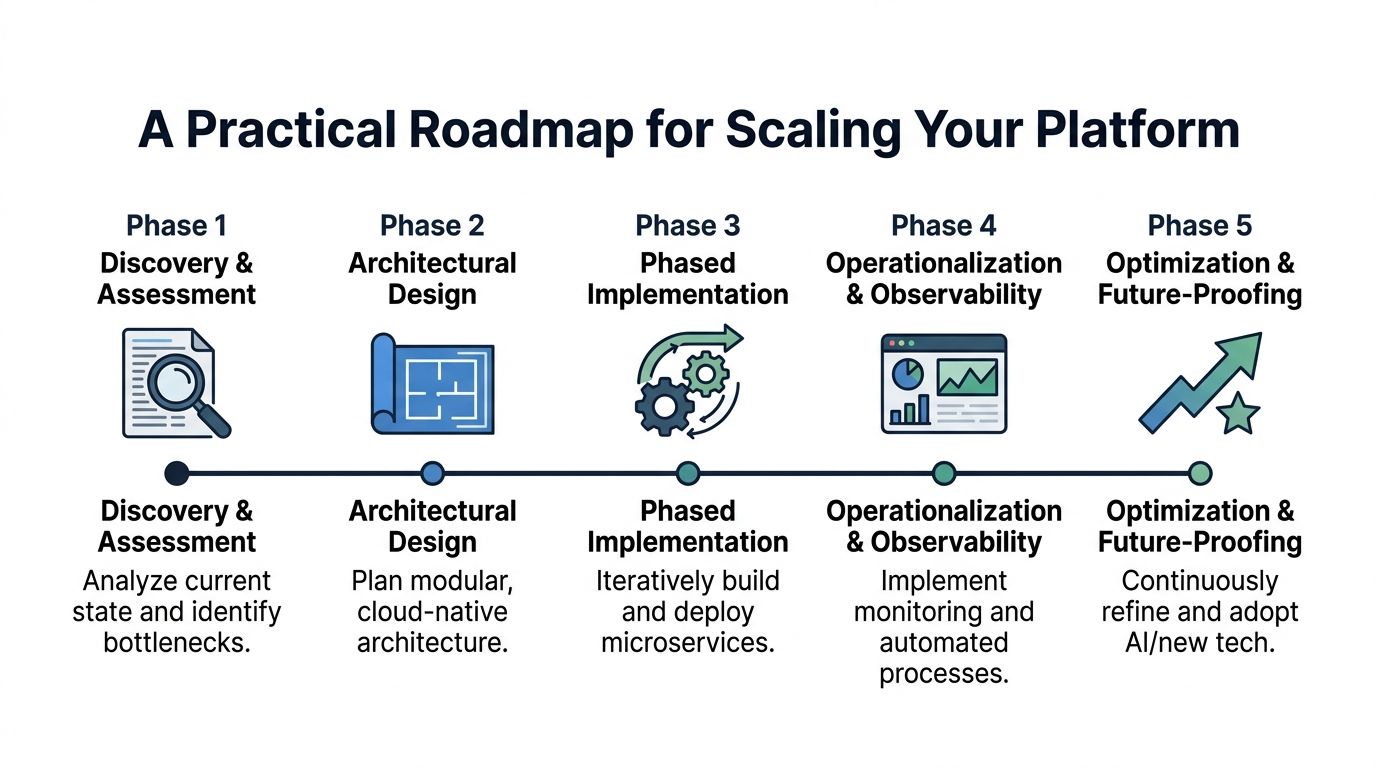
Phase one and two
In the earliest stage, don't chase architectural purity. Build a modular product with clear domain boundaries, strong access control foundations, and an interoperability plan that won't trap you later. A disciplined modular monolith is often enough if the team keeps modules explicit and avoids shared-database shortcuts across unrelated workflows.
Then move into deliberate architectural design. Here, teams define service boundaries, API contracts, audit requirements, and data governance rules before growth pressure forces reactive decisions.
Focus on these outcomes first:
A domain map that separates identity, consent, clinical data, messaging, and analytics concerns
A release model that supports safe change
A compliance baseline tied to actual system behavior, not policy documents alone
Phase three and four
The growth stage is where many platforms get messy. New customers bring custom requests. Sales pressure increases. The engineering team starts shipping exceptions instead of strengthening the foundation.
Resist that.
Move capabilities into services when there is a real reason: independent scaling, stronger security isolation, separate deployment cadence, or integration load that justifies it. At the same time, formalize CI/CD, observability, and incident response. Without those, service decomposition just creates a larger operational mess.
A sensible checkpoint list includes:
Interoperability maturity. Are FHIR and HL7 workflows reusable, versioned, and testable?
Operational readiness. Can on-call engineers trace a failure across services quickly?
Stakeholder adoption. Are clinical users trained on the workflows that are being scaled?
That last point matters more than many teams admit. Successful scalability requires coordinated stakeholder action, including equipping clinical staff through training and forming public-private partnerships to build secure shared data platforms, because technology alone isn't sufficient, as discussed in this PMC review of scaling remote patient monitoring tools.
Phase five
At enterprise scale, the conversation changes. Cost governance, resilience engineering, regional deployment strategy, and formal data governance become part of core platform management.
At this stage, teams should refine:
Disaster recovery design
Service ownership and SLOs
Consent and policy management across multiple organizations
Vendor and partner governance
If you need outside delivery support, Bridge Global is one option for teams aligning compliant platform engineering with an AI implementation roadmap. Their client cases can help benchmark what a phased delivery model looks like in practice.
FAQ on Healthcare Platform Scalability
When should a healthtech startup worry about scalability?
Earlier than most founders think. The signal isn't just rising user count. It's when the platform starts carrying workflows that can't tolerate ambiguity, such as patient communication, documentation, or cross-system data exchange. If your team is already handling incidents with manual fixes, direct database queries, or one-off interface patches, you have a scalability problem even if traffic still looks manageable.
Should a startup begin with microservices?
Usually not. Start with a modular architecture that keeps domain boundaries clear and avoids tight coupling. Move to microservices when you need independent scaling, stricter isolation, or independent deployment for specific capabilities. If a small team adopts many services too early, they often trade one kind of complexity for another.
What's the first technical warning sign that a platform is struggling to scale?
It usually shows up as unpredictability. A release changes one area and another area slows down. A partner integration creates side effects in unrelated workflows. Incidents take too long to diagnose because no one can trace the path across systems. Unpredictability is more dangerous than raw slowness because it tells you the team has lost clear control over system behavior.
How important is FHIR to healthcare platform scalability?
It's central if you expect to integrate across providers, devices, partners, or future product lines. FHIR won't remove all complexity, but it gives teams a shared structure for data exchange. Without that discipline, each new integration tends to introduce custom logic that becomes expensive to maintain.
Can serverless help in healthcare platforms?
Yes, in specific places. It's useful for bursty, stateless workloads such as event processing, scheduled jobs, or isolated integration tasks. It isn't a universal answer for every clinical workflow. Teams still need strong observability, explicit security boundaries, and careful handling of data movement involving PHI.
What compliance standards matter beyond HIPAA?
GDPR often becomes relevant when platforms touch users, data flows, or partnerships beyond the US. Many enterprise buyers also expect evidence of mature security operations and governance practices before procurement moves forward. The exact standards depend on your market, but the principle is consistent: compliance has to be designed into architecture and operations, not layered on during contract review.
How do you scale AI features safely in a clinical product?
Treat AI features as regulated operational components, not as isolated experiments. That means versioned models, governed training data, bias review, monitoring in production, and clear human escalation paths. It also means validating how the feature performs across languages, care settings, and underserved groups before broad rollout.
What's the biggest mistake CTOs make during healthcare platform growth?
They delay foundational decisions because the product is still moving fast. That usually means postponed data standardization, weak service boundaries, fragile integration design, and thin observability. Those shortcuts feel efficient early on. Later, they create the kind of expensive rewrite that leadership hoped to avoid.
If you're planning the next stage of healthcare platform scalability, Bridge Global can support the work with product strategy, compliant engineering, AI-enabled delivery practices, and cross-functional teams that build around interoperability, auditability, and operational resilience.
About Stephanie Cornelissen
Stephanie Cornelissen is a Technical Solutions Consultant with strong experience helping organizations navigate complex digital change. She works closely with teams to align business goals with practical, scalable technology solutions. With expertise in system architecture, integrations, and emerging technologies, she focuses on solving real-world problems through thoughtful execution. She enjoys working where technology meets business strategy and measurable growth.
View all posts by Stephanie Cornelissen →