


A Guide to Boosting Healthcare Interoperability Solutions
A lot of founders hit the same wall on their first serious healthcare integration project. The product works. The UI is clean. The customer wants a connection to an EHR, lab system, imaging platform, device feed, or payer workflow. Then the main problem shows up. Data can move, but it doesn't arrive in a form that clinicians trust or that teams can use.
That gap is where most interoperability projects get stuck.
Healthcare interoperability solutions aren't just about sending messages between systems. They're about making patient data available, understandable, governed, and usable inside real workflows. If you're building a platform for providers, payers, care management, remote monitoring, or digital therapeutics, you need to treat interoperability as product infrastructure, not a side integration task.
The good news is that the market has moved far beyond one-off interfaces. The hard part is that many teams still approach interoperability like a connector problem when it's instead a combined architecture, workflow, and governance problem.
Why Healthcare Interoperability Is No Longer Optional
A patient arrives in the emergency department and can't explain their medication history. Their recent labs sit in one system, allergy information in another, and imaging in a third. The hospital may have digital systems everywhere and still lack the one thing the care team needs in that moment: a complete, usable record.
That's why interoperability has shifted from a technical feature to core health infrastructure. The healthcare interoperability solutions market reached USD 4.9 billion in 2025 and is forecast to reach USD 12.5 billion by 2034, with a 10.72% CAGR from 2026 to 2034, according to IMARC Group's healthcare interoperability solutions market analysis. That projection matters because it reflects a broad move away from isolated clinical systems and toward integrated exchange across EHRs, HIEs, and API-based platforms.
The business case is operational, not theoretical
Disconnected systems create very practical problems:
-
Care teams lose time: They search across portals, PDFs, fax replacements, and portal exports instead of seeing the data in context.
-
Product teams build brittle workarounds: A custom parser solves one partner integration and breaks on the next.
-
Compliance risk grows: Data moves through ad hoc channels when official exchange paths are too slow or too limited.
-
New products stall: Patient apps, care coordination tools, and AI features depend on reliable access to structured data.
If you're building in this space, interoperability affects onboarding speed, implementation cost, product scope, and customer retention.
What buyers are really asking
Most healthcare buyers don't ask for “interoperability” in the abstract. They ask whether your product can pull medication lists, reconcile lab data, launch inside an EHR workflow, or support downstream reporting without manual cleanup.
Practical rule: If exchanged data still needs a human to reinterpret it before action, you don't have operational interoperability yet.
That's why choosing the right healthtech software development partner matters early. The integration strategy you choose at the first enterprise customer often shapes everything that follows, from architecture to implementation timelines to how easily you can add AI later.
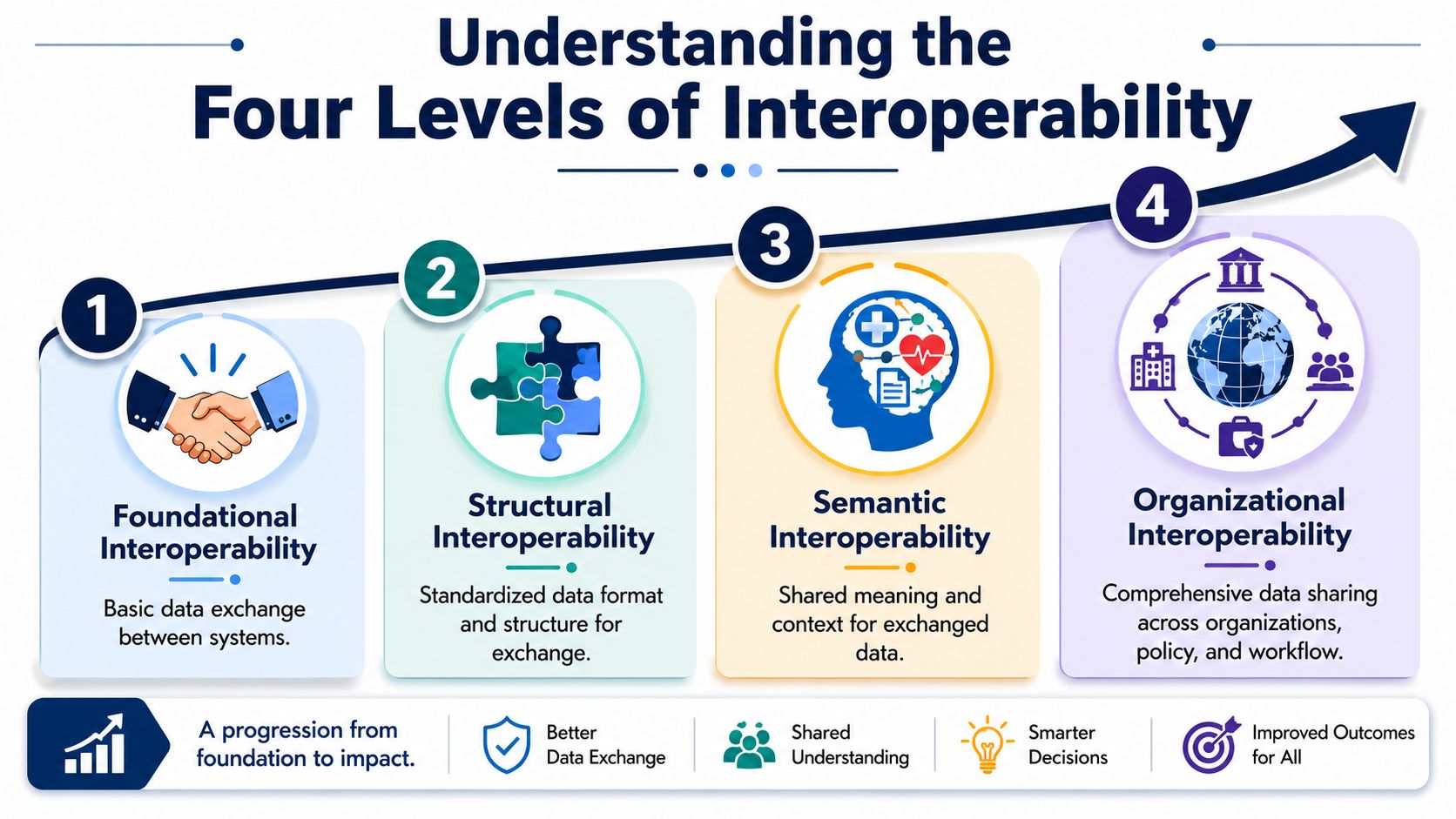
Understanding the Four Levels of Interoperability
Interoperability works like a stack. Each level solves a different problem, and teams get into trouble when they assume basic connectivity means the full stack is done.
By 2021, 96% of U.S. acute care hospitals had adopted certified EHRs, but only 62% were successfully operating across all four key interoperability domains, as summarized in these healthcare interoperability statistics. That difference is the clearest reminder that owning compliant software isn't the same as achieving reliable data exchange in practice.
Foundational and structural interoperability
The first two levels are about transmission and format.
Foundational interoperability means one system can send data to another. That's the minimum bar. A message arrives, a document is shared, an API responds.
Structural interoperability means the receiving system can parse the payload because the structure is predictable. Fields appear where they should. Data types are expected. Segments and resources follow agreed patterns.
These levels matter, but they don't create clinical value on their own. A medication can arrive as text and still be unusable if the receiving system can't map it correctly into a medication workflow.
Semantic interoperability
Semantic interoperability is where the data keeps its meaning after exchange.
This is the point where “glucose,” a local lab code, and a standard code are understood as the same clinical concept. It's also where units, terminology, and context stop breaking downstream workflows.
In product terms, semantic interoperability is the difference between “we ingested the record” and “our application can safely use the record.”
Shared data that lacks consistent meaning usually creates more work, not less.
Organizational interoperability
This is the hardest layer, and the one many startup teams underestimate.
Organizational interoperability includes policy, trust, consent handling, workflow alignment, operational ownership, and support processes across institutions. It answers questions like these:
-
Who authorizes access: Which party governs patient access and data release?
-
How are corrections handled: What happens when source data changes after exchange?
-
Where does reconciliation happen: In the EHR, your app, or a shared operational queue?
-
Who supports the interface: Your team, the provider IT team, the vendor, or an HIE participant?
Why the fourth level decides project success
A lot of projects reach level one or two, declare victory, and then stall in production. Data moves, but clinicians don't trust it. Operations teams can't resolve mismatches. Consent logic is unclear. Nobody owns terminology mapping. That's where timelines blow up.
If you review real-world client cases, the successful ones usually share the same pattern. The technology choice matters, but the delivery model works because workflow decisions and governance decisions are made early, not deferred until after integration testing.
Key Standards and Architectures Explained
Standards aren't interchangeable. Each one solves a different part of the problem, and using the wrong one for the wrong job creates expensive rework.
The current center of gravity is HL7 FHIR, because it supports an API-based approach that reduces integration friction compared with older messaging patterns. In practice, interoperability platforms often pair FHIR with DICOM for imaging and use SNOMED CT, LOINC, and ICD-10 for semantic normalization under HIPAA-aligned controls, as described in this review of heterogeneous health information systems.
What each standard is good at
A useful way to think about standards is as a toolkit, not a winner-take-all choice.
| Standard | Primary Use Case | Data Format | Key Advantage |
|---|---|---|---|
| HL7 v2 | Operational messaging between clinical systems | Message-based segments | Common in existing hospital workflows |
| CDA | Clinical document exchange | Structured XML documents | Good for document-style summaries |
| FHIR | App integration and API-based data access | Resource-based APIs and JSON or XML | Easier for modern application development |
| DICOM | Imaging exchange | Imaging files and metadata | Designed for radiology and imaging workflows |
| SNOMED CT, LOINC, ICD-10 | Terminology and coding normalization | Standardized vocabularies | Preserves shared clinical meaning |
HL7 v2, CDA, and FHIR in real projects
HL7 v2 is still everywhere. If you integrate with hospitals, labs, and older operational systems, you will encounter it. It’s proven and firmly embedded, but it wasn’t designed for the kind of developer-friendly, app-centric access most startups want.
CDA helps when the exchange unit is a clinical document rather than a live API interaction. It’s useful for summaries and formal document payloads, but it can feel heavy if your product needs granular, event-driven access.
FHIR is usually the right starting point for new product development because it supports modern web patterns. It’s better suited for patient apps, provider dashboards, population workflows, and embedded tools that need targeted resources rather than full document dumps.
That said, FHIR isn’t magic. Different vendors expose different resource sets, profiles, auth patterns, and implementation quirks. “Supports FHIR” can mean anything from a narrow patient read endpoint to a broader production-grade API estate.
Architecture that scales and architecture that breaks
Point-to-point integrations look fast at the start. They rarely stay manageable. Each new partner adds another custom mapping path, another support burden, another versioning problem.
A better pattern is open standards plus an integration platform. That usually means a normalization layer between your product and external systems, strong canonical data models, and clear versioning rules. It also means planning for healthcare integrations as a platform capability instead of a sales-driven exception.
For many teams, that architecture becomes part of a broader custom healthcare software development strategy. If your product spans patient engagement, clinical workflows, reporting, and partner APIs, interoperability can’t live as a sidecar.
Don’t ask whether a vendor “supports FHIR.” Ask which resources, which write operations, which auth model, which versioning policy, and how they handle terminology mapping.
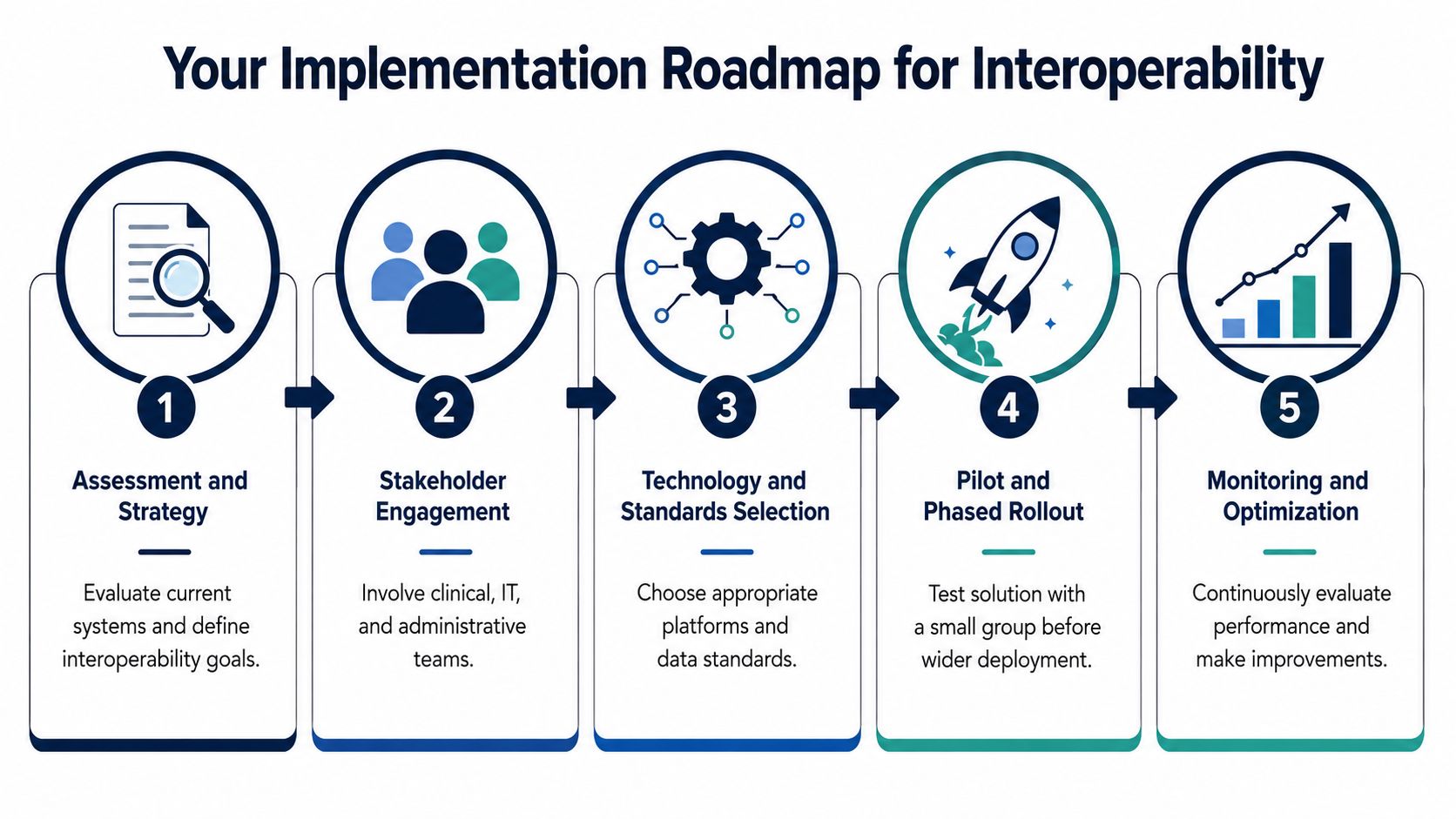
Your Implementation Roadmap for Interoperability
Most interoperability failures don’t happen because the standard was wrong. They happen because the team skipped discovery, under-scoped workflow complexity, or tried to modernize everything at once.
Research described practical deployment as “profoundly fragmented and inconsistent,” especially around legacy systems, in athenahealth’s discussion of interoperability challenges in healthcare. That lines up with what product and engineering teams see in the field. The legacy environment is usually the project.
Start with workflows, not interfaces
Before choosing an engine, API gateway, or data model, map the workflow you’re trying to improve.
Ask basic but uncomfortable questions:
-
What clinical or operational action should happen once data arrives?
-
Which system is the system of record for each data domain?
-
Where do humans intervene when data conflicts?
-
Which exchange paths are required at launch, and which can wait?
If a founder tells me, “We need FHIR integration,” I usually translate that into a narrower implementation question. “Which workflow is blocked because the right data isn’t available at the right time?”
Build the roadmap in phases
A practical roadmap often looks like this:
-
Assessment first: Inventory source systems, required data objects, auth constraints, partner dependencies, and current failure points.
-
Narrow scope: Pick one high-value workflow such as patient intake, medication history, lab reconciliation, or referral handoff.
-
Canonical model next: Define how your platform represents core entities before mapping inbound and outbound partner data.
-
Pilot before scale: Launch with a limited set of users, partners, or departments and watch where the operational edges break.
-
Govern after go-live: Create ownership for mappings, exception handling, audit trails, and consent logic.
Legacy systems need adapters, not denial
Founders often ask whether they should replace the customer’s old systems. Usually, they can’t. And they don’t need to.
The more realistic approach is to isolate legacy complexity behind adapters, transformation layers, and integration services. That lets your product interact with a stable internal model while you handle partner-specific variance at the edge. It’s slower at the beginning than a direct custom connector, but much safer by the third or fourth integration.
A managed delivery approach can help if your team doesn’t have in-house integration depth. For example, teams evaluating delivery structure should compare implementation ownership, partner management, and long-term maintenance before choosing a model such as this full-cycle delivery model guide.
Testing has to match production reality
Interoperability testing isn’t just schema validation. You need to test for real-world conditions:
-
Missing fields: Source systems won’t always send complete data.
-
Duplicate records: The same event may arrive twice through different paths.
-
Terminology drift: Local codes can change without warning.
-
Workflow timing: Data that arrives late can be as harmful as data that never arrives.
If you’re building a new platform or extending an existing product, interoperability planning should sit inside the same delivery process as your SaaS product development. Otherwise, the core app and the integration layer evolve in different directions.
How to Select the Right Interoperability Partner
Founders often compare vendors by demo quality or implementation price. That’s understandable and usually wrong.
The right partner for healthcare interoperability solutions needs depth in standards, yes, but also discipline in delivery. An integration can pass technical validation and still fail because the partner doesn’t understand clinical workflows, production support, or how to manage exceptions after launch.
What to test during vendor evaluation
Use the sales process to expose how the partner works.
-
Ask for implementation specifics: Have them walk through a real FHIR or HL7 integration lifecycle, including mapping, validation, auth, testing, and post-launch support.
-
Probe legacy experience: Ask how they connect to systems that don’t expose clean modern APIs.
-
Review terminology handling: See whether they treat semantic mapping as a first-class task or an afterthought.
-
Check operating model: Find out who owns interface monitoring, issue triage, and change management when a source system updates.
-
Validate compliance habits: Security controls and HIPAA-aligned practices should show up in design, logging, access control, and deployment choices.
Red flags that cost time later
Some partners talk confidently about standards but stay vague on implementation details. That’s a warning sign.
Watch for these patterns:
-
“We support all standards” without naming resource coverage, message types, or terminology constraints.
-
Custom connector enthusiasm with no plan for reuse or internal abstraction.
-
No clear support boundary between your app, their middleware, and the provider’s source system.
-
Workflow blindness, where the technical team ignores how nurses, administrators, billers, or physicians will use the output.
If a vendor can’t explain how bad data gets quarantined, reconciled, and corrected, they’re not ready for production healthcare.
Match the engagement model to the product stage
If your roadmap includes broader platform work beyond integrations, compare a pure interoperability vendor with a partner that can also deliver custom software development. The right choice depends on whether interoperability is an isolated project or part of a larger product build.
It also helps to review different software development service models before committing. A startup with one major customer integration may need a different arrangement from a scale-up building a repeatable enterprise onboarding engine.
Bridge Global is one example of a partner model that combines healthcare engineering, product delivery, and AI-enabled software work. That matters if your interoperability layer is tied to the rest of the platform rather than standing alone.
The Future Is Now AI-Driven Interoperability
AI becomes useful in interoperability when it solves messy problems that rules alone don’t handle well. That usually means unstructured content, inconsistent terminology, noisy inbound data, and prioritization across large data flows.

Where AI already adds value
A few patterns are emerging as practical, not speculative:
-
Clinical note extraction: NLP can pull structured concepts from free-text notes, discharge summaries, and referral narratives.
-
Terminology assistance: ML-assisted mapping can help normalize local codes against standard vocabularies, though it still needs human oversight.
-
Record summarization: AI can organize fragmented records into clinician-friendly views when the underlying data arrives from multiple sources.
-
Operational triage: Models can help prioritize interface errors, detect unusual payload changes, and flag records likely to fail downstream workflows.
The key is to keep AI downstream of a solid interoperability foundation. If your source data is unstable and your governance is weak, AI will amplify inconsistency faster than it creates value.
What responsible adoption looks like
The safest sequence is simple. Standardize exchange first. Normalize key concepts next. Introduce AI where humans are currently spending too much time on repetitive interpretation or cleanup.
That might mean using AI development services to support note structuring, coding support, data quality checks, or event prioritization. For larger organizations, the conversation usually expands into broader enterprise AI solutions and a staged AI implementation roadmap, so model behavior, data handling, and governance evolve together.
Where founders should be careful
Don’t pitch AI as a substitute for standards. It isn’t.
AI helps most when it operates on top of clear data contracts, stable workflows, and accountable review paths. In healthcare, a “smart” integration that nobody can audit will lose trust quickly. If you’re exploring hospital operations use cases, this AI and hospital automation whitepaper is a useful companion to interoperability planning because it focuses on where automation fits into operational healthcare environments.
Frequently Asked Questions About Interoperability Solutions
Is FHIR enough to make systems interoperable?
No. FHIR is often the right transport and API layer for modern products, but interoperability also depends on terminology mapping, workflow design, access policies, testing, and support ownership. Teams that treat FHIR as the whole solution usually end up with technically valid exchange and operational confusion.
What’s the biggest mistake startup teams make?
They scope around the interface and not around the workflow. A founder might ask for patient data sync, but the actual requirement is medication reconciliation before a clinical action, or lab ingestion before a triage decision. If the workflow isn’t defined, implementation expands in every direction.
How should we handle legacy EHR environments?
Don’t force replacement unless the customer is already committed to it. Use adapters, transformation services, and a canonical internal data model, so your application stays stable while partner-side complexity is isolated. That approach is less glamorous than a clean-sheet rebuild, but it’s usually the one that survives production.
How much should governance matter in an early-stage product?
A lot more than often expected. Beyond technical integration, organizational interoperability requires shared consent models, secure communication, and data governance and policy interventions as core enablers, especially when data moves between providers, devices, and consumer apps, according to Meditech Insights’ healthcare interoperability solutions market discussion.
That shows up in practical decisions such as who can access what, how patient consent is represented, how records are corrected, and how audit history is preserved.
Can we prove ROI before we scale?
Yes, but keep the proof narrow. Pick one workflow where bad data handoffs are already visible, such as intake, referrals, or lab review. Measure operational friction qualitatively if you don’t yet have strong instrumentation. The fastest path to value is usually one painful workflow done well, not a broad but shallow exchange.
Should we buy a platform or build our own layer?
Teams often need both. Buy what’s a commodity, such as infrastructure components, interface tooling, or specific integration services. Build the parts that define your product, your workflow advantage, and your data model. If every mapping and routing decision lives in a vendor black box, product differentiation gets harder over time.
How do consent and trust affect cross-organization exchange?
More than most integration plans acknowledge. Even when systems can technically exchange data, projects slow down when organizations disagree on permissible access, patient authorization, or responsibility for downstream use. Trust isn’t a soft issue in healthcare. It directly shapes architecture, contracts, support processes, and whether users will rely on the result.
As we explored in our guide to healthcare software strategy, the strongest products in this space don’t separate architecture from operations. They design for both from the start.
If you’re planning your first major interoperability project, Bridge Global can support the work as a technology partner for healthcare product engineering, integrations, and AI-enabled software delivery. The useful starting point is usually a scoped discovery that identifies the workflow, source systems, standards fit, and governance gaps before implementation begins.
About Upendra Jith
Upendrajith completed his Master's in English and has been a commercial content developer for the past three years. He's more inclined to develop content with a 'street-smart' delivery on topics such as technology, media, or anything he can get his hands on. He has a fixation on lyrics, dark poetry, media, technology, and flow arts.
View all posts by Upendra Jith →