


Your Guide to Healthcare Application Modernization Services
The most popular advice on healthcare modernization is also the most dangerous. It treats the project like a technology refresh. Move to the cloud, rebuild the UI, expose some APIs, and declare victory.
That framing misses the underlying problem. In healthcare, legacy applications aren’t just expensive to maintain. They create operational fragility inside clinical workflows that can’t tolerate confusion, delay, or bad data. If your scheduling, lab, billing, and EHR-adjacent systems are brittle, your modernization program should be judged by one standard first. Does it reduce clinical risk while improving day-to-day flow?
That’s why serious leaders don’t buy healthcare application modernization services as a coding exercise. They buy them to lower disruption, tighten control, improve interoperability, and create a safer path for future change. If you need a healthtech software development partner, start with one that understands clinical operations, not just architecture diagrams.
Beyond Tech Debt Modernizing: to Reduce Clinical Risk
Most boards still approve modernization for the wrong reason. They hear “technical debt” and think the IT team wants cleaner code. Clinicians hear “new system” and expect workflow disruption. Both sides miss the point.
Healthcare modernization should be framed as an operations and safety program. Industry coverage on healthcare system modernization makes that clear: the highest-risk question isn’t which stack you pick, but how to modernize without disrupting clinical operations or patient safety, and success depends as much on clinician adoption, data migration strategy, and phased rollout as on the technology stack itself, as noted by Particle41’s healthcare modernization analysis.

What legacy risk actually looks like
A legacy platform rarely fails in one dramatic way. It fails through accumulation.
-
Workflow friction: Staff create workarounds because the system doesn’t match how care is delivered.
-
Data inconsistency: Information lands in one module but doesn’t reliably reach the next team.
-
Change paralysis: Leaders delay necessary updates because even minor changes might trigger downstream issues.
-
Security exposure: Old components and weak controls increase compliance and operational stress.
Those problems don’t stay in IT. They spill into patient access, discharge coordination, prior authorization, revenue integrity, and clinician trust.
Practical rule: If your modernization plan starts with infrastructure and ends with workflow validation, your priorities are backwards.
The better way to define modernization
Modernization means making healthcare systems safer to operate, easier to change, and more reliable under real clinical load. That includes application redesign, integration cleanup, security hardening, testing discipline, and rollout control. It also means giving operators confidence that an improvement in one area won’t break another.
Leaders who get this right usually treat modernization as part of enterprise risk management. Security, compliance, and release control belong in discovery, not after build. Bridge this thinking with governance early, especially if your roadmap includes AI-enabled workflows. A useful reference is this whitepaper on AI regulatory compliance and security for MedTech.
If your team still describes the effort as “upgrading old software,” reset the language. You’re redesigning the conditions under which care operations run.
The Urgent Case for Healthcare System Modernization
The biggest mistake in healthcare modernization is treating urgency as an IT problem. It is a patient safety and operations problem first.
Legacy systems fail in ways that look routine until they disrupt care. A delayed interface update means a clinician works from stale information. A brittle scheduling flow creates access bottlenecks that staff patch by phone and spreadsheet. An unpatched dependency turns a small security issue into an outage, an audit problem, or both. Delay does not preserve stability. It preserves exposure.
That is why organizations investing in custom healthcare software development usually act after the cost of inaction becomes obvious. The trigger is rarely a desire for newer technology. It is repeated downtime, failed integrations, weak release confidence, rising support burden, or workflows that depend on heroics from a few experienced employees.
Security and compliance pressure
Healthcare leaders should stop separating modernization from compliance. In older environments, access rules drift, logging is inconsistent, and no one has a clean view of how protected data moves across systems. That creates audit risk and operational risk at the same time.
A sound modernization program starts with security architecture, identity and access design, logging, traceability, and change control. Those decisions belong in discovery and planning, not after build. If a vendor can explain cloud migration but cannot explain how they will handle regulated data flows, approval paths, and evidence collection, they are not ready for healthcare. That is why focused cyber compliance solutions matter. You need controls designed for clinical systems under regulatory pressure.
Interoperability failures slow care operations
Hospitals and health systems run through connected applications. EHR integrations, lab systems, billing tools, scheduling platforms, patient portals, imaging workflows, and departmental software all have to work together under daily load. Legacy environments often hold that together with brittle interfaces and undocumented fixes.
When applications are disconnected, staff fill the gaps manually. Orders get re-entered. Teams reconcile records across screens. Support queues fill up with data-mismatch issues that should never reach end users. This is not just an efficiency problem. It increases the chance that the right information does not show up in the right place at the right time.
A disconnected set of applications does more than waste labor. It weakens trust in clinical and operational data.
Patient experience is a back-end reliability issue
Executives often fund the front end first because patients can see it. That misses the true source of failure. Portals, digital intake, self-scheduling, and billing communication only work when the underlying systems stay accurate and available.
Patients do not care whether the problem started in a monolith, an aging integration engine, or a broken batch process. They experience the result. Appointments look wrong. Messages arrive late. Bills conflict with what the staff said earlier. If the back end is unstable, the patient experience will be unstable too.
Operational drag shows up in margin and morale
Legacy applications consume time, money, and management attention long before anyone approves a replacement budget. Release windows stretch because testing is manual and dependencies are unclear. Support risk concentrates around a few people who know how the old system really works. Teams avoid useful changes because rollback is painful and outage risk is hard to predict.
The pattern is easy to recognize:
-
Slow change cycles: Routine updates require too many handoffs, approvals, and workarounds.
-
Support concentration: Critical knowledge sits with a small number of people.
-
Low release confidence: Teams delay improvements because failure is hard to contain.
-
Workflow compensation: Staff uses calls, spreadsheets, and side processes to keep care and billing moving.
A modernization program should reduce those failure modes. If it does not lower operational risk, improve release control, and remove manual compensations from clinical workflows, it is not modernization. It is a costly infrastructure exercise with very little business value.
Core Modernization Strategies and Architectural Patterns
Not every legacy system should be rebuilt. That mistake burns budget and raises risk. The right modernization strategy depends on how tightly the application is coupled to clinical workflows, how risky change is, and how much future flexibility you need.
Healthcare application modernization services need real judgment. The “5 Rs” are useful, but only if you treat them as a decision framework rather than a menu.
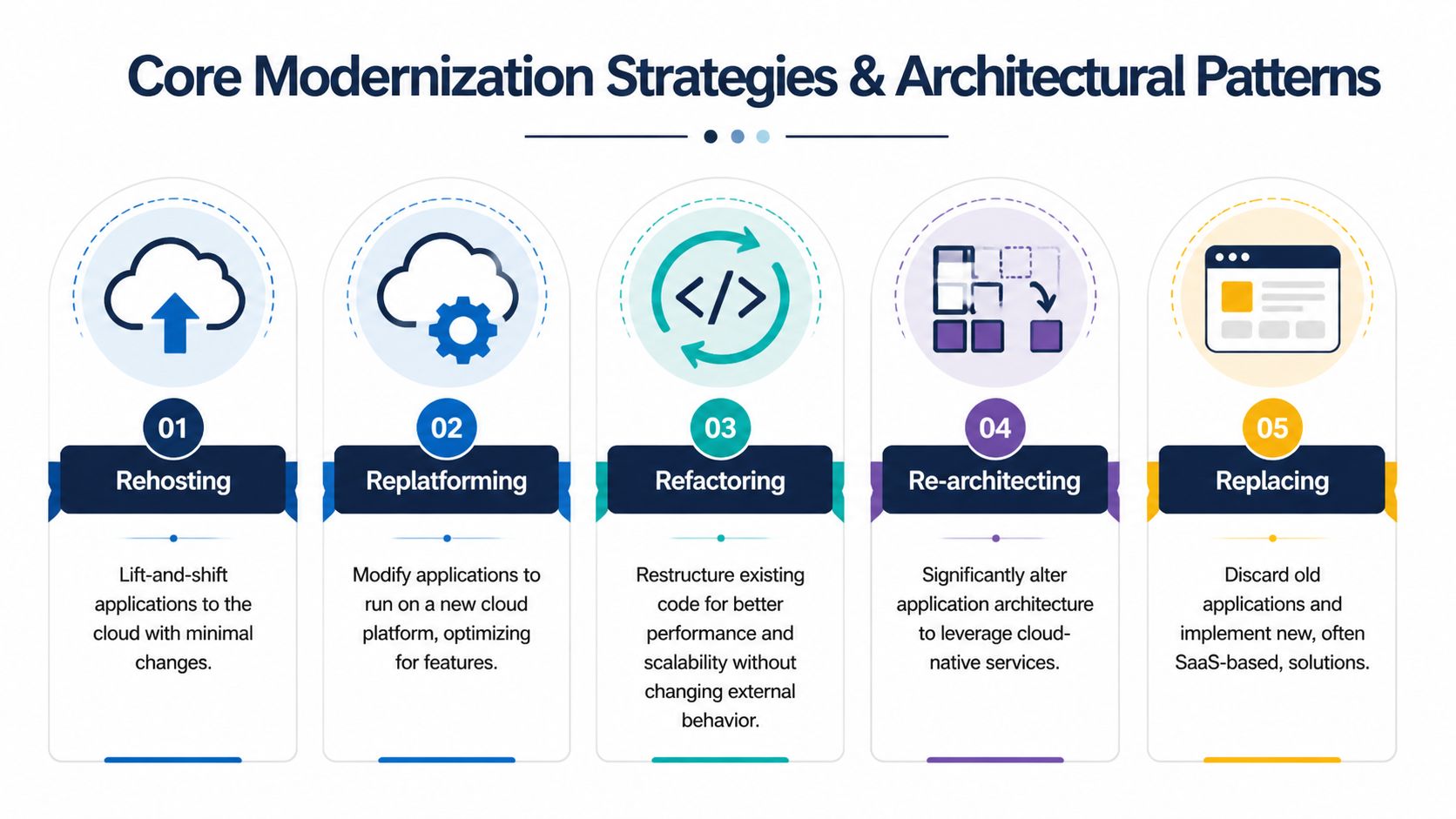
Comparison of the 5 Rs of application modernization
| Strategy | Description | Typical Use Case | Risk/Effort | Cloud Impact |
|---|---|---|---|---|
| Rehost | Move the application with minimal code change | Infrastructure refresh, urgent hosting exit | Lower code risk, limited transformation value | Moves workload to cloud infrastructure quickly |
| Replatform | Make targeted platform changes without rewriting core behavior | Improve operability, use managed services | Moderate effort | Better use of cloud platform capabilities |
| Refactor | Restructure code to improve maintainability and scalability | Application has value but poor internal quality | Higher engineering effort | Supports more resilient cloud operation |
| Re-architect | Change core structure to support modular or cloud-native design | Monolith blocks delivery speed and integration | High effort and design complexity | Enables deeper cloud-native benefits |
| Replace | Retire the old application and implement a new product or SaaS solution | Legacy app no longer fits business or compliance needs | High organizational change risk | Depends on replacement platform |
Why rip-and-replace is usually the wrong call
A full cutover sounds clean on slides. In hospitals, it often creates concentrated risk. The safer pattern is incremental replacement, where teams extract one bounded capability at a time, keep it behind existing APIs, and run legacy and modern components in parallel until behavior is validated. That approach reduces patient-care disruption and helps preserve data consistency, regulatory compliance, and uptime during migration, as described in Arpatech's healthcare cloud-native modernization guidance.
That model works because it respects how healthcare systems behave in production. Real workflows involve exceptions, strange edge cases, old business logic, and human habits that never show up in requirements documents.
The pattern I'd recommend most often
For most provider organizations, the best path is a strangler-style modernization pattern. Keep the monolith in place. Carve off a bounded capability such as appointment reminders, intake, eligibility workflow, document handling, or rules-heavy billing logic. Put the new component behind a stable interface. Validate it against live behavior. Then move to the next capability.
Use this approach when:
-
The legacy system still contains critical business logic that can't be safely rewritten all at once.
-
Clinical uptime matters more than architectural purity.
-
Teams need rollback control and side-by-side validation before full switchover.
-
The organization wants measurable progress instead of a long blackout period with uncertain payoff.
Support the pattern with automated testing, infrastructure-as-code, release controls, and solid cloud services. Those practices aren't optional. They're the mechanics that make incremental change survivable.
Don't modernize the entire estate at once. Modernize one dependency chain at a time.
How to choose among strategies
Ask three direct questions:
-
Is the application strategically important? If yes, preserve flexibility.
-
Is the workflow risk high? If yes, avoid big-bang replacement.
-
Is the current problem technical, operational, or product-level? That answer usually tells you whether to refactor, re-architect, or replace.
A hosting problem is not a rebuild problem. A workflow problem is not fixed by rehosting. A compliance problem may require replacement or architectural redesign. Teams fail when they use one answer for every application.
The Technical Blueprint for Modern Healthcare Systems
A healthcare architecture earns its value by reducing failure points in care delivery and making daily operations easier to run. If the stack is hard to control, hard to test, or hard to integrate, it becomes a clinical risk.
Cloud choices should follow workflow and risk
Cloud decisions should start with service impact, not vendor preference. Ask which workloads need tighter recovery controls, which ones create upgrade bottlenecks, and which ones waste staff time because they are expensive to maintain.
Use a simple operating model:
-
IaaS fits when you need to stabilize a legacy application, preserve control, and improve backup, recovery, and environment consistency before a deeper redesign.
-
PaaS fits when the goal is faster delivery, less platform maintenance, and stronger standardization for new services and APIs.
-
SaaS fits when the workflow is common across the industry and owning the application adds little strategic value.
The wrong cloud model creates new operational drag. The right one improves release control, observability, incident response, and audit readiness.
Interoperability has to be engineered
Interoperability is not a procurement item. It is a set of design decisions about data ownership, message standards, validation rules, API boundaries, and error handling.
Healthcare systems break down when interfaces grow one project at a time without a governing model. Teams end up with fragile point-to-point integrations, duplicate patient data, and workflow delays that clinicians feel long before IT logs the ticket. A better blueprint defines canonical data models, standard integration patterns, and clear ownership for every interface.
FHIR is useful because it supports modern application access to clinical data. HL7 v2 will remain in many environments for years. The technical goal is not to force purity. It is to reduce interface sprawl, make integrations easier to test, and lower the odds of silent data mismatches.
AI belongs after the platform becomes trustworthy
Many healthcare organizations chase AI while their core systems still produce inconsistent data and unstable workflows. That is a mistake. Bad inputs and weak controls turn AI into an error amplifier.
AI starts paying off after identity, integration, data quality, and workflow reliability are under control. Then it can support focused use cases such as scheduling optimization, documentation support, coding review, triage assistance, and revenue operations. For revenue operations specifically, this guide to RCM AI for clinics is a useful outside reference because it ties AI decisions to workflow, denials, and reimbursement pressure.
Digital transformation consulting matters for sequencing, governance, and tradeoff decisions.
Modern architecture should reduce operational variance first. Then it can support AI safely.
QA is part of patient safety
Testing in healthcare modernization is not a release formality. It is one of the controls that prevents patient matching errors, broken order flows, access issues, and billing defects from reaching production.
That is especially true in custom healthcare software development, where one change can affect multiple systems, roles, and downstream processes. I would require four testing layers before any major cutover:
-
Automated regression testing for high-volume clinical and administrative workflows
-
Data validation testing across source systems, target systems, and interface mappings
-
Role-based access testing for privacy, segregation of duties, and operational control
-
Parallel-run validation to compare new behavior against live legacy outcomes before retirement
If a vendor can demo screens but cannot explain rollback criteria, test coverage, reconciliation rules, and defect containment, do not trust them with a modernization program.
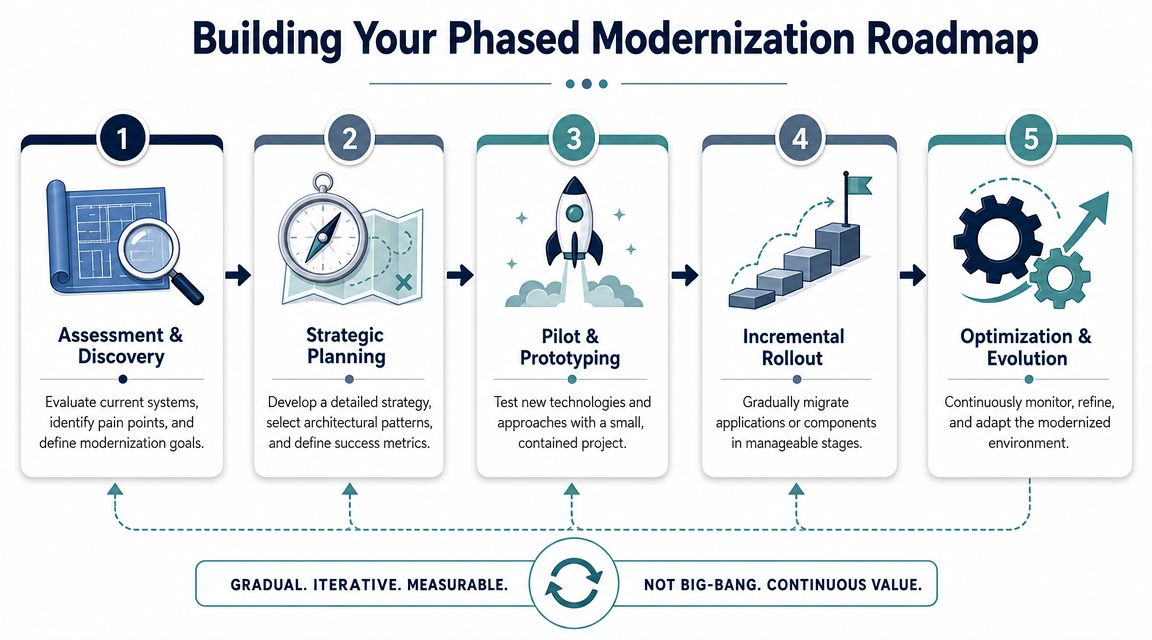
Building Your Phased Modernization Roadmap
If your roadmap fits on one optimistic slide, it's probably wrong. Healthcare modernization needs a sequence, not a slogan.
The first phase is not migration. It's assessment. A robust modernization program begins with a full system audit and dependency mapping because legacy clinical platforms often contain hidden coupling, outdated libraries, and compliance gaps that aren't visible from the UI or API layer alone. Inventorying applications and tracing data flows across environments helps teams target the highest-risk modules first and build a safer roadmap, as explained in Sisgain's guidance on healthcare app modernization.
Phase 1 starts with reality, not ambition
Before anyone talks about target architecture, get a verified picture of the current estate.
That means documenting:
-
Application inventory: Which systems are active, which are historical, and which are “temporary” tools that became permanent.
-
Dependency chains: How data moves across EHR, labs, billing, scheduling, and departmental tools.
-
Operational criticality: Which modules can fail subtly and which ones immediately affect care flow.
-
Compliance exposure: Where access, retention, audit, or transmission controls may be weak.
This exercise usually reveals more shadow logic than teams expect. It also stops leaders from funding the wrong first move.
Sequence for risk reduction, not optics
A good roadmap doesn't start with the most visible app. It starts with the most impactful, lowest-blast-radius opportunity. Sometimes that's an integration layer. Sometimes it's a scheduling workflow. Sometimes it's a brittle back-office component that causes endless downstream rework.
I prefer a phased model that looks like this:
-
Assess and map the current environment in enough detail to identify hidden coupling.
-
Stabilize the riskiest components with security and operational controls.
-
Pilot one bounded modernization target with clear rollback and validation.
-
Expand incrementally based on dependency order, not executive preference.
-
Optimize after each release instead of waiting for a mythical finish line.
This is where digital transformation consulting actually matters. Not for buzzwords. For sequencing, governance, and tradeoff decisions.
Define value in operational terms
Traditional ROI models are too narrow for healthcare modernization. You should absolutely track engineering efficiency and support burden, but that's not enough. The stronger case comes from operational outcomes.
Measure value through questions like these:
-
Are teams spending less effort on manual reconciliation?
-
Are releases more predictable?
-
Is clinical workflow less exposed to system instability?
-
Can leadership approve changes with more confidence?
-
Has the environment become easier to secure and audit?
The fastest way to lose support for modernization is to promise transformation and deliver only platform churn.
If you want quick wins, earn them through contained improvements that users can trust. Then use that trust to tackle harder systems.
Your Vendor Selection Checklist for Modernization Success
Most vendor selection processes overweight presentation quality and underweight delivery discipline. In healthcare, that's a bad way to buy modernization.
You need a partner that can operate inside ambiguity, regulated workflows, messy integrations, and organizational resistance. Nice slides don't prove any of that.

What to evaluate before you sign
Use a checklist that focuses on outcomes and the operating model, not just certifications.
-
Healthcare delivery context: Ask whether the team understands clinical workflow risk, not only compliance language.
-
Integration depth: Confirm practical experience with healthcare data exchange patterns, interface cleanup, and interoperability work.
-
Migration methodology: Require a phased model with validation, rollback, and parallel-run controls.
-
Security posture: Look for embedded security review, not an isolated final audit.
-
Team composition: Make sure architects, QA, DevOps, and delivery leads are all present from the start.
-
Post-launch support: Modernization isn't finished at go-live. You need stabilization, optimization, and operational support.
Questions that expose weak vendors fast
Ask these in the first serious meeting:
| Question | What a strong answer sounds like |
|---|---|
| How do you handle hidden dependencies in legacy healthcare systems? | They describe discovery, dependency mapping, and production validation. |
| How do you reduce cutover risk? | They talk about phased rollout, rollback paths, and parallel validation. |
| How do you test regulated workflows? | They explain role-based, integration, and data validation testing. |
| What happens after launch? | They have a support and optimization model, not just a handoff. |
If responses stay generic, walk away.
Evaluate fit, not just capability
Some organizations need a strategic advisor. Others need a build partner with embedded delivery. Others need augmentation through a dedicated development team. The right model depends on your internal bench strength and governance maturity.
For teams that want a structured path from discovery through delivery, options can include custom software development, product engineering services, and an AI transformation framework if the long-term roadmap includes intelligent workflow automation. Bridge Global is one example of a provider that combines those models with healthcare-focused delivery and broader AI for your business planning. For due diligence, ask any shortlisted partner to show relevant client cases.
Operational leaders should also pressure-test whether the vendor understands revenue cycle dependencies, because modernization often breaks at the billing edge. For additional perspective from outside the software vendor ecosystem, these Happy Billing insights for RCM are useful when you want to evaluate how front-end application changes ripple into billing performance.
Buy the team that can explain your failure modes before they propose your future state.
Frequently Asked Questions about Healthcare Application Modernization
What are healthcare application modernization services?
They’re services that help healthcare organizations update legacy applications in a controlled way so systems become easier to operate, integrate, secure, and change. In practice, that can include architecture redesign, cloud migration, API strategy, data migration, testing, workflow validation, and phased rollout support.
Should hospitals replace everything at once?
No. That approach concentrates risk. A phased program is safer because teams can isolate one bounded capability, validate it, and preserve rollback options before moving further.
What should happen before any code changes?
A full audit and dependency mapping exercise. If you skip that, you’ll miss hidden couplings, shadow logic, and compliance gaps that only show up after migration work starts.
How do you know which application to modernize first?
Start with the component that creates serious operational drag or risk but has a manageable blast radius. Good first targets are often integration-heavy functions, brittle workflow components, or systems that create repeated manual reconciliation.
Is cloud migration the same as modernization?
No. Cloud migration may be part of modernization, but moving a bad application into a new environment doesn’t fix workflow flaws, poor architecture, or weak interoperability. Sometimes rehosting is useful. It’s not a complete strategy by itself.
Where does AI fit in a modernization program?
After the core platform becomes reliable enough to support it. AI depends on stable workflows, trustworthy data, and clear governance. If those foundations are weak, AI initiatives usually create more noise than value.
What should executives expect from a vendor?
They should expect a phased method, clinical-risk awareness, strong QA discipline, rollback planning, and post-launch support. If the vendor can’t explain how they’ll protect operations during change, they’re not ready for healthcare.
How long does modernization take?
It depends on the application estate, the level of coupling, and the rollout model. What matters more than calendar length is whether the plan creates visible progress without exposing clinical operations to avoidable disruption.
If you’re planning a major modernization effort, Bridge Global can support the work from discovery through delivery with healthcare-focused engineering, AI-enabled development practices, and pragmatic modernization planning built around risk control, interoperability, and operational continuity.
About Preethi Saro Philip
Preethi Saro Philip is a Post Graduate Research Degree holder in Economics with more than 10 years of experience in writing, editing, research and teaching. She has an intense passion for content crafting and calls herself a ‘wordsmith’. She enjoys writing on wide-ranging topics including business, technology, health & lifestyle, education, environment etc.
View all posts by Preethi Saro Philip →