


Connected Healthcare Platforms: A Guide for Teams
Connected healthcare platforms have moved from a growth bet to a core infrastructure decision in digital health. Market forecasts point to rapid expansion over the next few years, but the more important signal for product teams is operational. Care delivery now depends on systems that can keep device data, clinical workflows, and patient interactions in sync over time.
That changes the architecture brief.
A connected platform has to support continuous care, not just isolated transactions. It needs to absorb data from devices and third-party systems, route it into the right workflow, and present the right context to clinicians and patients without turning every release into another custom integration effort.
Teams that succeed usually make one strategic choice early. They treat the platform as a long-term operating model for care and service delivery, not as a collection of features. This architectural shift is why choosing a capable healthtech software development partner matters early, especially when decisions about interoperability, security, and scaling will shape both clinical reliability and commercial flexibility from day one.
The Unstoppable Rise of Connected Healthcare
Connected care is no longer a pilot concept. As noted earlier, the market outlook points to sustained growth, but the more useful signal for builders is operational. Health systems, payers, and digital care companies are redesigning service delivery around continuous data exchange, not one-off encounters.
That changes what a platform has to do.
Healthcare could live with fragmented systems when a visit ended the transaction. That assumption fails in remote monitoring, hospital-at-home, chronic disease management, and post-discharge follow-up, where data keeps arriving after the appointment, and different teams need the same patient context. If the architecture cannot connect those signals reliably, clinical staff compensate with phone calls, spreadsheets, inbox triage, and duplicate data entry.
Connected healthcare platforms address that gap by giving teams a shared operating layer for patient data, workflow events, and communication history. For product teams, the strategic question is not whether to add connected features. It is how to design the platform so each new integration improves the model instead of increasing maintenance costs. That is why healthcare platform API engineering decisions belong near the start of platform planning, not near the end.
Why the market signal matters
Growth in this category matters because it reflects a structural change in buying and care delivery.
Three shifts show up repeatedly in platform programs:
-
Care pathways now extend beyond the clinic: Remote follow-up, medication adherence, and device-based monitoring all depend on reliable data flow across time.
-
Users judge the experience as one service: Patients do not care which vendor owns scheduling, messaging, RPM, or pharmacy updates. They notice whether the experience feels connected and whether care teams have context.
-
Buyers scrutinize integration risk earlier: Procurement questions now reach architecture fast. Can the platform handle device feeds, identity matching, consent controls, auditability, and EMR integration without custom work for every client?
Practical rule: If your roadmap assumes manual reconciliation between systems will remain acceptable, the roadmap is already behind.
In practice, manual reconciliation is not an abstract process problem. It is a nurse keying blood glucose readings from a patient logbook into the EMR because the glucometer does not sync. It is a care coordinator comparing discharge notes from one portal against medication data in another system before calling the patient. It is a support team exporting CSV files to match device alerts with the right patient account because identifiers do not line up across systems. Those workflows absorb clinical time, introduce avoidable errors, and make scale expensive.
What teams often get wrong
First-time platform teams often start with the surface layer. They ask for video visits, device sync, dashboards, alerts, and a patient app. Those capabilities matter, but they do not create a durable platform by themselves.
The harder work sits underneath. Identity resolution, consent handling, event routing, interoperability standards, data normalization, and workflow configuration determine whether the product supports real care operations or just displays information in more places.
I have seen teams ship attractive front ends that failed during implementation because each customer required a different integration pattern, a different patient matching rule, and a different exception process for missing data. At that point, every new feature becomes slower to release and harder to trust. A connected healthcare platform earns its value when the architecture can absorb those differences without forcing clinicians and operations teams to patch the gaps by hand.
Understanding the Core Architecture
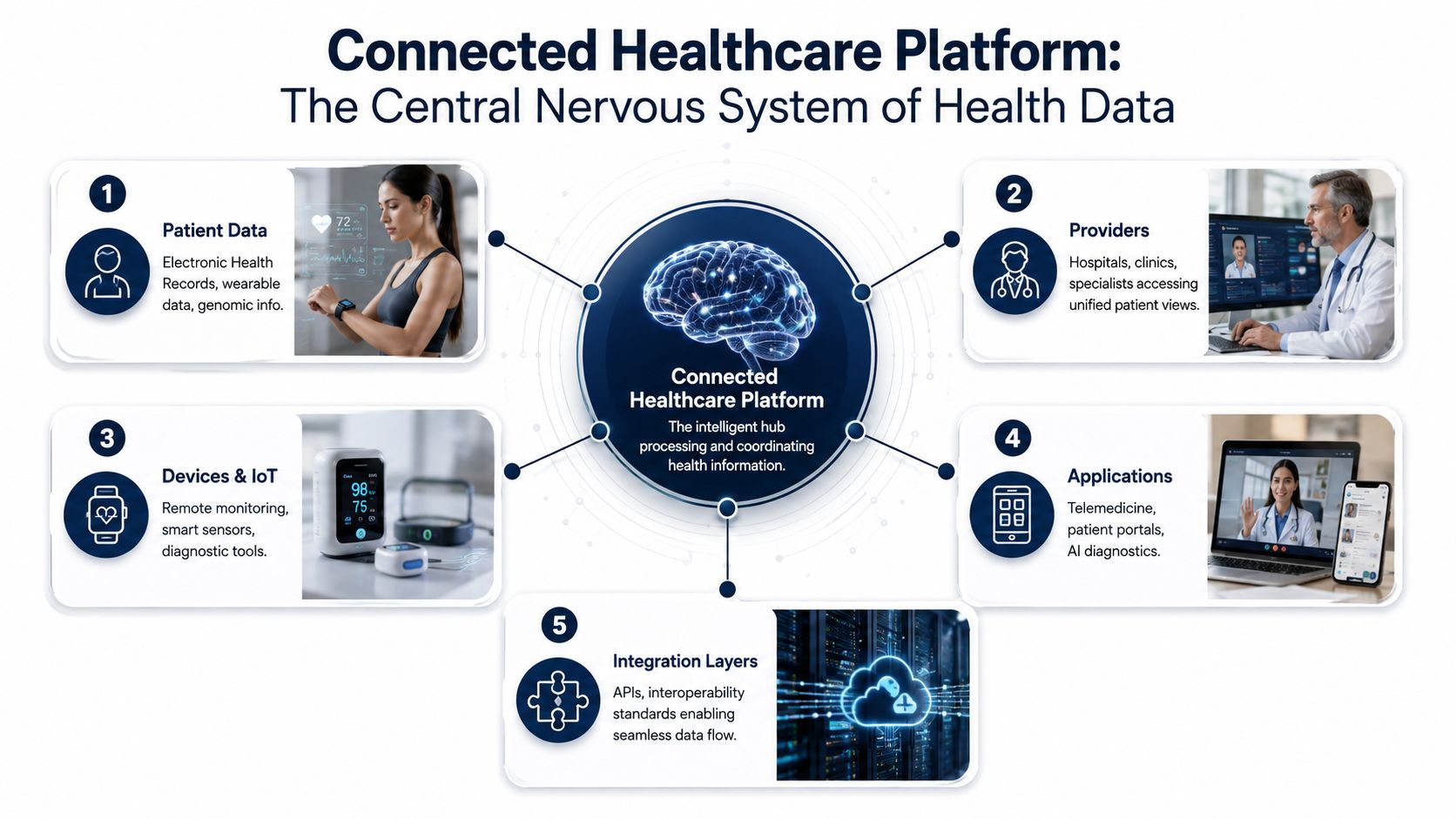
A connected healthcare platform works like a central nervous system for clinical and operational data. It receives inputs from different sources, translates them into a usable form, and routes them securely to the right people and systems. That's the architectural job. Everything else sits on top of it.
Connected healthcare platforms are modular, cloud-based systems that store, normalize, and securely route heterogeneous clinical data. This architecture eliminates data silos by unifying patient information and communication points for care teams, as described in Cleffex's overview of connected healthcare platforms.
What the platform actually does
At the architecture level, the platform has three core jobs.
| Function | What it means in practice | Why it matters |
|---|---|---|
| Store | Collect data from records, devices, prescriptions, and communications | Preserves a usable patient history |
| Normalize | Convert different formats and protocols into a common model | Makes analytics, automation, and care workflows possible |
| Route securely | Send the right data to the right user or subsystem with controls | Protects privacy and reduces clinical friction |
Normalization is the part many teams underestimate. Device data doesn't arrive in a clean, uniform structure. Wearables, bedside devices, mobile apps, and external systems all speak differently. A useful platform translates that raw input into standardized resources and events that downstream products can trust.
Why modular beats tightly coupled
Modularity isn't a buzzword here. It's what lets you evolve the platform without breaking the whole thing. Device ingestion, identity, audit logging, notifications, analytics, and clinical workflow services should be separable enough to change independently.
That doesn't always mean a full microservices estate on day one. It does mean clear domain boundaries. If appointment logic, consent rules, and device telemetry processing all live in one tangled code path, every release becomes a compliance and regression risk.
A good reference point is thinking through API boundaries early, especially for third-party exchange and internal service separation. We explored that in our guide to healthcare platform API engineering.
The architecture should make new integrations boring. If every new partner requires custom handling across the entire stack, the core design is wrong.
A simple example
Suppose a patient uses a Bluetooth blood pressure monitor, receives an e-prescription update, and messages a care coordinator through a portal. Those events shouldn't land in three separate systems with three separate identities and audit trails. The platform should unify them under one patient context, standardize the data, and expose it through clinician dashboards, alerts, and downstream analytics.
That's the difference between software that connects things and a platform that supports care.
Essential Components of a Connected Platform
Most connected healthcare platforms fail for predictable reasons. Not because they lacked ideas, but because one foundational layer was weak. In practice, the platform needs a set of components that reinforce each other. If one is fragile, the user experience becomes fragile too.
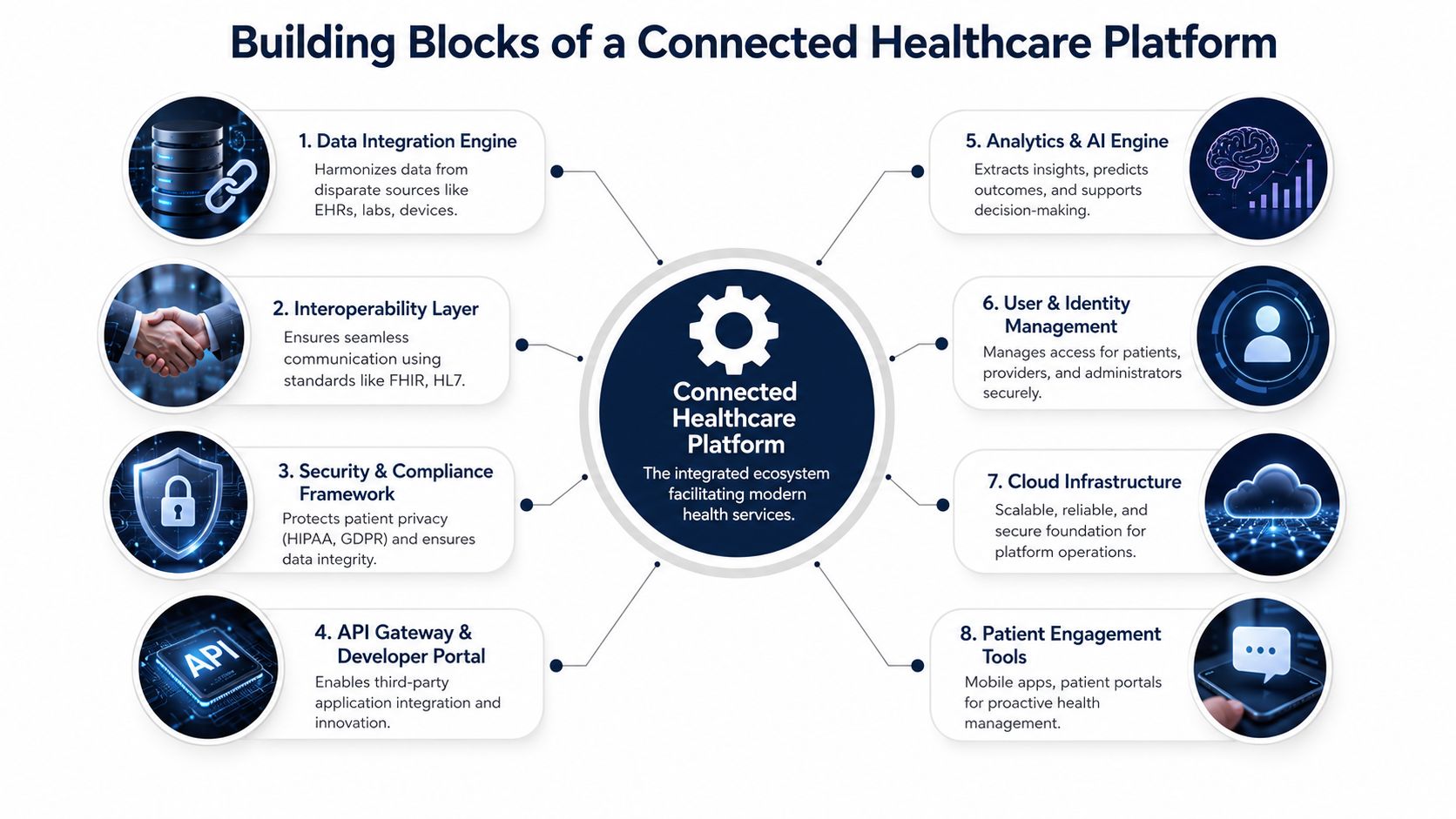
Interoperability first
For real-time clinical data exchange, FHIR is the mandatory, developer-friendly approach with strong regulatory momentum, especially for patient-facing applications and new system implementations, according to Murphi's healthcare interoperability standards guide. HL7 still matters, especially when older hospital systems are involved, but new platform work should treat FHIR as the primary language at the edges.
That means your interoperability layer should do more than pass through payloads. It should validate, transform, version, and monitor them.
Key capabilities here include:
-
FHIR resource handling: Patient, Observation, MedicationRequest, Encounter, and related clinical objects.
-
Legacy translation: HL7 and vendor-specific mappings where older systems still dominate.
-
Terminology alignment: Consistent code sets and validation logic.
-
Operational monitoring: Clear visibility into failed messages, retries, and schema drift.
As we explored in our guide to healthcare integrations, interoperability work isn't separate from product strategy. It is product strategy.
Identity and access control
In healthtech, access design is a clinical safety decision as much as a security decision. Nurses, specialists, device admins, support staff, patients, and external partners all need different scopes. That model has to be explicit.
To ensure IoT compliance within connected healthcare ecosystems, platforms must implement role-based access controls (RBAC) and multi-factor authentication (MFA) for high-risk devices, while aligning with frameworks like the HIPAA Security Rule and NIST CSF 2.0, as outlined in Cylera's IoT compliance guidance for healthcare.
A secure baseline usually includes:
-
RBAC by default: Define access around role and workflow, not convenience.
-
MFA for sensitive actions: Especially for admin functions, device management, and privileged access.
-
Auditability: Every critical action should be traceable.
-
Device trust controls: High-risk endpoints need stronger policy enforcement.
If your team is evaluating infrastructure posture and hosting implications, ARPHost's HIPAA compliance guide is a useful operational resource because it translates compliance expectations into concrete hosting and environment decisions.
Device connectivity and data movement
Remote monitoring, diagnostics, and home-based care depend on reliable ingestion from devices and apps. Teams often create hidden technical debt in this area. They connect one device model, hard-code assumptions, and call the ingestion layer done. That doesn't scale.
A healthier pattern is to build a general device gateway with adapters. Normalize early, tag provenance, and preserve raw events where needed for audit or later analysis. The same rule applies to data pipelines. Design for retries, delayed delivery, duplicate messages, and partial failure.
Our guide to healthcare data fabric for unifying siloed data is relevant here because the biggest platform problem usually isn't missing data. It's unmanaged data fragmentation.
AI and engagement layers
Analytics and AI only produce value when upstream data is clean enough to trust. That's why I'd place AI after interoperability, identity, and pipeline design, not before. Once the foundation is sound, AI development services can support triage, documentation assistance, anomaly detection, and patient-specific recommendations.
Patient engagement tools also belong in the core stack, not as a late add-on. Portals, messaging, reminders, digital intake, and telehealth touchpoints are how patients experience the platform. If those tools aren't tied to the same identity, workflow, and clinical context as the backend, the system feels disconnected no matter how good the architecture looks on paper.
Navigating Benefits and Real-World Challenges
Connected healthcare platforms promise better coordination, more visibility, and smoother patient experiences. They can deliver all of that. But they also expose weaknesses that point solutions can hide for years. That's why platform planning has to balance upside against delivery risk.
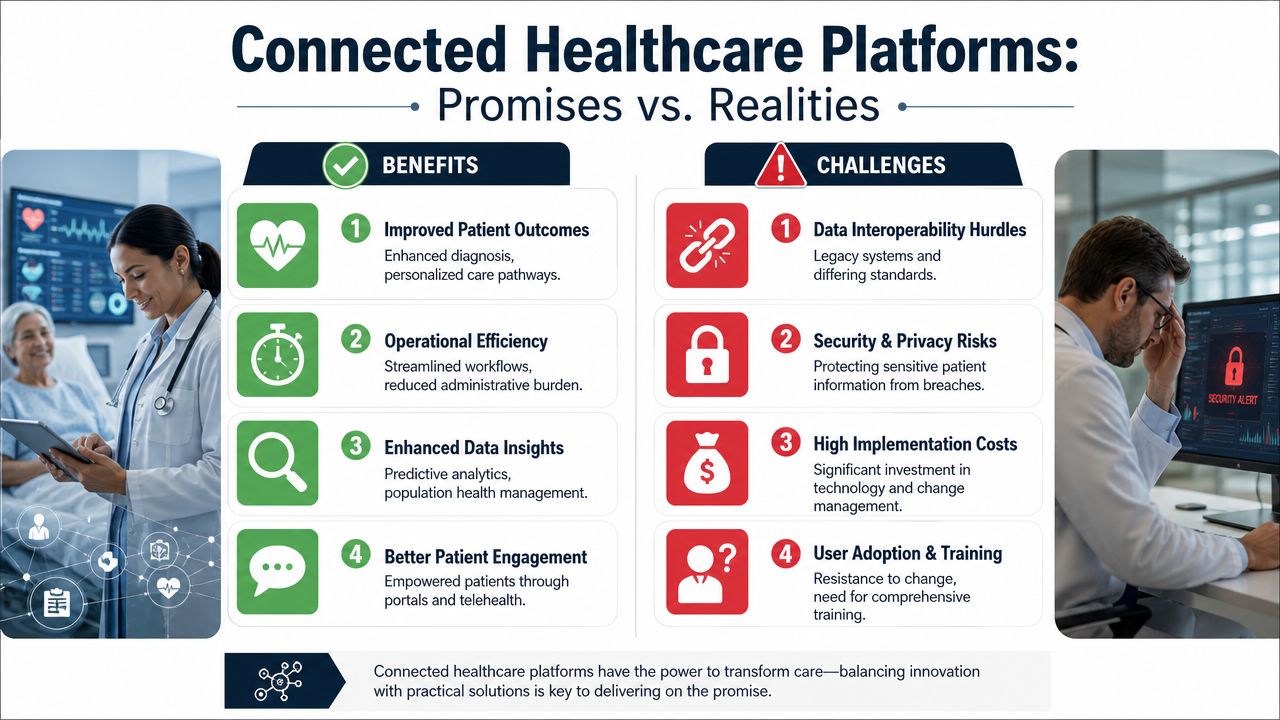
Where the benefits show up first
The earliest value usually appears in operations. Care teams get a more coherent patient view. Admin staff spend less time reconciling systems. Product teams gain a cleaner foundation for adding services without rebuilding identity and data flows every quarter.
There's also a direct patient effect when the platform is designed well:
-
Better continuity: Information follows the patient more reliably.
-
Cleaner communication: Messaging, alerts, and follow-up workflows live in one system.
-
More usable insight: Clinicians can act on current signals instead of stale snapshots.
-
Less app sprawl: Patients don't need to guess which tool handles which task.
In organizations investing in enterprise AI solutions, those gains can extend into documentation support, triage assistance, and workflow orchestration, provided the underlying platform is structured for it.
Where reality pushes back
The hardest problems are rarely the ones in a demo. They show up in access, trust, compliance, and adoption.
A critical challenge is the Infrastructure & Trust Gap. Up to 60% of eligible rural patients may not engage with platforms due to a lack of devices, reliable internet, or trust, and new regulations are mandating pre-visit digital readiness checks, a feature missing in 70% of current SaaS vendor offerings, according to this ScienceDirect analysis on digital readiness and underserved care.
That should change how teams define “patient onboarding.” In underserved settings, onboarding isn't just account creation. It includes checking whether the patient has a usable device, stable connectivity, audio and video capability, enough privacy to participate, and confidence in the app itself.
Don't confuse technical availability with practical access. A telehealth feature that a patient can't confidently use is still unavailable care.
Compliance pressure is broader now
Security still matters in the usual ways, but accessibility has become a hard delivery requirement too. Under the HHS final rule effective July 8, 2024, connected healthcare platforms and third-party tools must meet WCAG 2.1 Level A and AA standards for digital accessibility, and organizations of 15 or more employees must comply by May 11, 2026, as summarized in Patient Partner's healthcare accessibility compliance article.
That means accessibility can't sit in a design QA checklist at the end. It affects component libraries, form behavior, navigation patterns, color contrast, and media workflows from the start.
Practical friction you should expect
| Promise | What actually happens if you underbuild |
|---|---|
| Unified patient experience | Patients face fragmented logins and inconsistent workflows |
| Better clinical efficiency | Staff create side processes to compensate for missing integration logic |
| More equitable access | Rural and underserved users drop off before first meaningful use |
| Smarter automation | AI outputs are ignored because source data isn't trusted |
One practical mitigation is to reduce interaction burden for clinicians and patients wherever possible. Voice can help here, especially for note capture and hands-busy workflows. If you're evaluating options, this overview of healthcare voice recognition technology is a useful companion resource because it frames the trade-offs around documentation and usability rather than treating voice as a novelty feature.
A Phased Implementation Roadmap for Healthtech Teams
First platforms fail when teams try to launch the full vision all at once. A connected healthcare platform needs sequencing. You need enough architecture discipline to avoid rework, but not so much abstraction that delivery stalls before users ever touch the product.
Remote Patient Monitoring is projected to dominate the application segment with a 33.5% share in 2026, which makes it a strong candidate for an MVP focused on chronic condition workflows, according to Coherent Market Insights' connected healthcare market report.

Phase one through three
Discovery and strategy
Start by narrowing the clinical and business problem. Don't begin with “build a connected health platform.” Begin with a specific outcome such as remote hypertension management, post-discharge follow-up, or medication workflow coordination.
During discovery, define:
-
Primary users: Patients, clinicians, care coordinators, device admins, support staff.
-
Core workflow: What event starts the process and what action closes it.
-
Required systems: EHR, pharmacy, payer, device vendors, messaging services.
-
Compliance scope: Privacy, audit, accessibility, identity, consent.
This is also where architecture choices begin. Many early products can start with a modular monolith if the team is small and the domains are still moving. What matters is clean boundaries. A monolith with clear modules is healthier than premature microservices with weak ownership.
Pilot and prototype
Use the MVP to validate one meaningful connected workflow. RPM is often the right place because it combines device data, clinical review, alerts, and patient engagement in a measurable loop.
A useful pilot usually includes:
-
A focused patient cohort
-
One or two supported devices
-
A clinician review dashboard
-
Alerting and escalation rules
-
Basic audit and access controls
Avoid building a marketplace, analytics suite, and broad partner ecosystem during the pilot. Those can come later. Early success depends on proving that a single workflow can run reliably from ingestion to action.
Build the smallest workflow that proves the platform can move from data capture to clinical action without manual glue.
Platform development and integration
Once the pilot is stable, strengthen the parts that will support scale. To achieve this, teams should invest in interoperability services, identity, audit logging, notification infrastructure, and reusable workflow components.
A strong pattern is to harden these horizontal capabilities before expanding feature breadth. If you skip that step, every new care program recreates the same plumbing.
Our guide to healthcare data pipeline architecture is a good lens for this stage because data movement becomes the limiting factor once the product starts integrating more sources and actions.
Phase four and five
Deployment and rollout
Rollout isn't just technical deployment. It includes operational onboarding, training, support, and escalation ownership. Decide who responds to device failures, who triages missing data, and who owns access-change requests. If no one owns those issues, clinicians absorb the burden.
This is also the stage where many teams realize their user model was too simplistic. External specialists, temporary staff, and patient proxies often need controlled access patterns that weren't modeled in the prototype.
Optimization and expansion
After launch, expand carefully. Add adjacent workflows that reuse the core platform rather than creating isolated modules. E-prescribing, digital intake, follow-up messaging, and care coordination are common next steps if the initial RPM program is solid.
For teams building a product rather than a single internal system, this is also where commercial packaging starts to matter. Multi-tenant architecture, configuration controls, tenant-specific integrations, and deployment repeatability become central. That's where experience in custom healthcare software development, an AI implementation roadmap, and disciplined SaaS product development can materially reduce rework.
Build versus partner decisions
Not every capability should be built from scratch. Teams should usually own the clinical workflow layer, user experience, and core data model decisions. They can often partner for infrastructure acceleration, selected integrations, or AI components.
One practical option in this space is Bridge Global, which works across custom software development, AI-enabled engineering, and regulated product delivery. That matters when a team needs both platform thinking and execution support, not just staff augmentation.
Measuring Success and Choosing Your Development Partner
A connected healthcare platform isn't successful because it launched on time. It's successful when clinicians keep using it, patients complete the workflows it enables, and operators can scale it without inventing manual workarounds.
The most persuasive success measures sit at the intersection of clinical, operational, and product performance. You don't need a huge KPI catalog. You need a small set of indicators that reflect whether the platform changed how care is delivered.
What to measure
The right scorecard depends on the workflow, but teams generally should track outcomes across four lenses:
-
Clinical workflow adoption: Are care teams using the platform as the default path, or bypassing it?
-
Patient engagement quality: Are patients completing setup, responding to prompts, and staying active in the program?
-
Operational reliability: Are integrations, alerts, and role-based workflows running without constant human intervention?
-
Administrative efficiency: Is the platform reducing documentation and coordination burden?
Artificial intelligence is one of the clearest ROI levers when it is embedded into the right workflow. It can reduce administrative burden by 30-40% in hospital settings by automating care coordination and clinical documentation, and EMR or clinical documentation holds a 36.26% solution share, according to Grand View Research's connected healthcare platform market report.
That doesn't mean every product needs AI on day one. It means you should identify where repetitive coordination, summarization, or documentation work is slowing the system down and decide whether AI can responsibly remove friction there.
How to evaluate a development partner
A good partner for connected healthcare platforms should be able to discuss architecture trade-offs without hiding behind generic transformation language. Ask how they handle FHIR boundaries, auditability, device ingestion, accessibility, and release management in regulated environments. If they can't talk through those details clearly, the risk will show up later in the build.
Use a short evaluation checklist:
| Evaluation area | What to look for |
|---|---|
| Healthcare domain depth | Experience with clinical workflows, compliance boundaries, and interoperability realities |
| Delivery flexibility | Clear software development service models that match product stage and internal team structure |
| Engineering breadth | Ability to cover backend, cloud, QA, UX, data, and AI where needed |
| Proof of execution | Relevant client cases that show comparable complexity |
Pick the partner who helps you reduce system risk, not the one who promises the longest feature list in the shortest timeline.
The wrong partner will optimize for visible output. The right one will protect the architecture, challenge weak assumptions, and help you ship something that remains supportable after launch.
Frequently Asked Questions
What’s the difference between a connected healthcare platform and a point solution?
A point solution does one job well. It might handle scheduling, virtual visits, or a single remote monitoring workflow. A connected healthcare platform supports multiple workflows on shared foundations such as identity, interoperability, audit, data routing, and patient context.
That distinction matters because point solutions often become expensive to maintain as soon as you need cross-workflow visibility. Platforms cost more to design carefully, but they create a cleaner base for expansion.
Where does blockchain fit in connected healthcare platforms?
Blockchain is usually not the platform core. It’s more relevant when you need stronger traceability, tamper-evident records, or trust models that cross organizational boundaries. In connected healthcare, that can matter for data integrity and drug traceability.
The mistake is trying to use blockchain as a substitute for good platform architecture. It isn’t a replacement for FHIR, workflow design, consent management, or access control. It’s a specialized layer for particular trust and provenance needs.
What should a startup do first if it wants to build in this space?
Start with one narrow workflow and map every data handoff inside it. Identify the users, systems, consent points, and failure states. Then define the minimum platform capabilities required to run that workflow safely and repeatedly.
A startup should also make compliance part of product design immediately. That includes access control, auditability, accessibility, and interoperability assumptions. If those are postponed, the rework usually lands at the worst possible moment, right when buyers start asking harder questions.
If you’re planning your first connected health product or modernizing an existing one, Bridge Global can support the architecture, integration, AI, and delivery decisions that turn a promising concept into a usable platform.
About Stephanie Cornelissen
Stephanie Cornelissen is a Technical Solutions Consultant with strong experience helping organizations navigate complex digital change. She works closely with teams to align business goals with practical, scalable technology solutions. With expertise in system architecture, integrations, and emerging technologies, she focuses on solving real-world problems through thoughtful execution. She enjoys working where technology meets business strategy and measurable growth.
View all posts by Stephanie Cornelissen →