


AI Chatbots for Patient Support: A Strategic Guide
The market for healthcare chatbots was estimated at US$1,202.1 million in 2024 and is projected to reach US$4,355.6 million by 2030, with a 24.0% CAGR from 2025 to 2030, according to Grand View Research’s healthcare chatbots market analysis. That matters because patient support is no longer a side feature. It’s becoming part of the operating model for providers, digital health platforms, and care programs.
In a demonstration, the process is clear. A patient asks a question, the bot replies, and everyone nods. Production is different. A real patient support chatbot has to authenticate users, protect PHI, connect to scheduling and records systems, route edge cases to staff, and stay within clinical and regulatory boundaries. That’s where many projects slow down or fail.
AI chatbots for patient support can work well when the scope is disciplined. They’re strongest in repetitive, high-volume interactions such as scheduling, reminders, medication information, navigation, refill workflows, and post-visit follow-up. They struggle when teams expect them to act like autonomous clinicians, improvise with weak source content, or serve every patient group equally well without targeted testing.
Builders need a full-lifecycle view. Product strategy, HIPAA design, conversation safety, integration architecture, rollout sequencing, and measurement all have to align. If you’re evaluating a healthtech software development partner, this is the level of detail worth asking for before any build starts.
The Rise of AI Chatbots in Modern Healthcare
Nearly one in five medical group practices had already put chatbots or virtual assistants into patient communication by 2025, as noted earlier. That level of adoption matters for one reason. Patient support has become an operations problem, not just a digital front-end feature.
The pressure is easy to see inside provider organizations. Contact centers are handling scheduling requests, refill questions, directions, intake steps, portal confusion, and post-visit follow-up at the same time, and staffing remains tight. A patient support bot is often the first AI project that survives budget review because it maps to existing service queues, existing cost centers, and existing patient pain points.
In production, these systems do more than answer common questions. They sit inside portals, SMS flows, mobile apps, and call deflection paths. They identify intent, collect the minimum data needed to move a workflow forward, and pass the case into scheduling, CRM, EHR, or nurse triage systems when automation should stop.
That distinction matters.
A demo bot can answer ten polished prompts. A production bot has to authenticate users correctly, avoid exposing PHI in the wrong channel, log consent where needed, and hand off to staff without losing context. Teams that pair a chatbot work with custom healthcare software development usually get more practical value because the bot becomes one part of a connected service layer rather than a disconnected widget.
The programs that mature fastest usually pair automation with feedback collection. Tools such as Open-source patient feedback tools help teams see where patients get stuck, which intents fail repeatedly, and which responses create confusion or drop-off. That feedback loop is one of the clearest differences between a pilot that looks promising and a support channel that keeps improving after launch.
The broader shift is operational. Ownership usually moves out of a single innovation or marketing team and into a working group that includes product, engineering, compliance, security, clinical operations, and integration leads. In healthcare, that is the point where a chatbot stops being a novelty and starts becoming part of the service infrastructure.
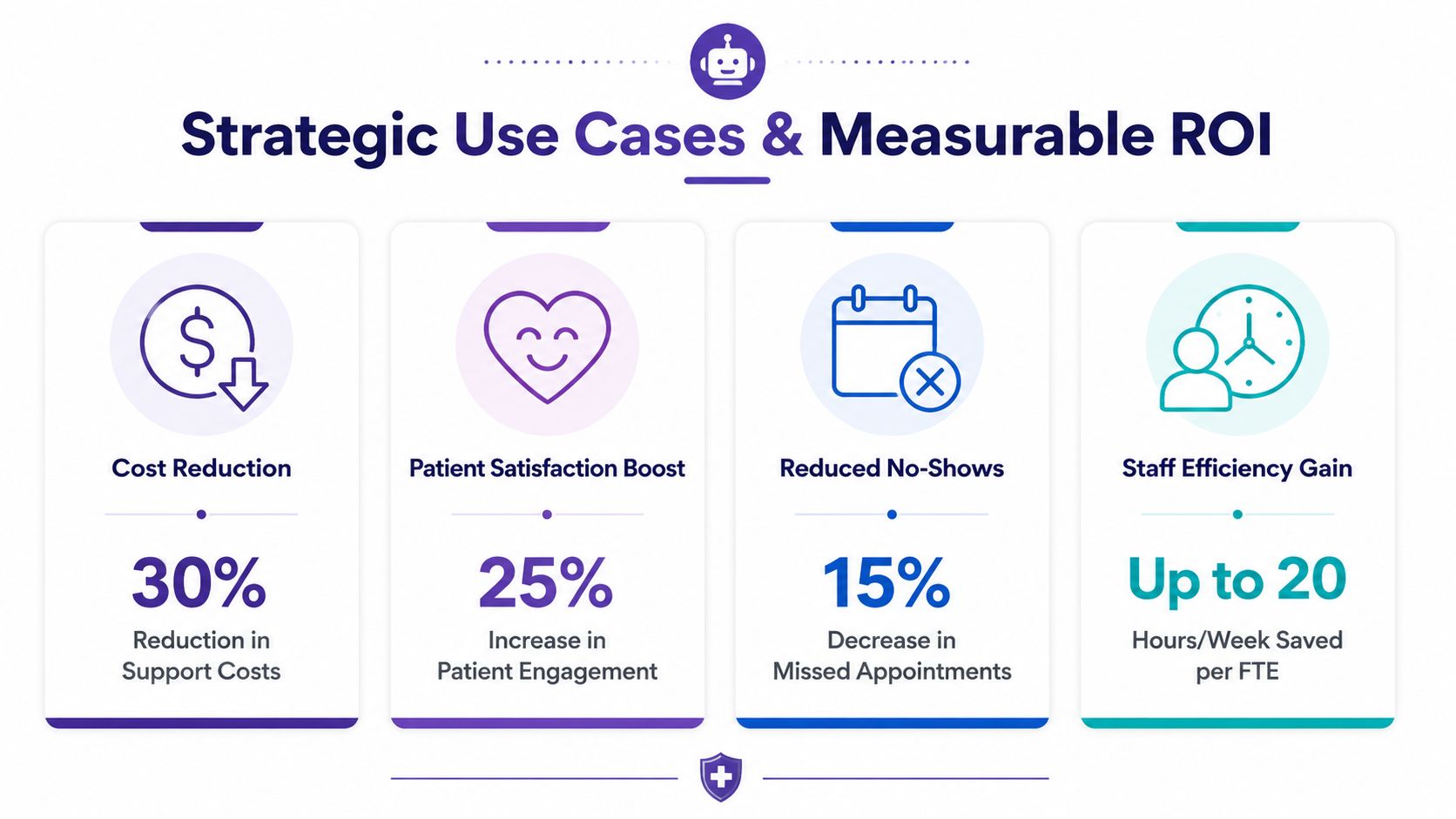
Strategic Use Cases and Measurable ROI
The most valuable chatbot projects start with one narrow operational problem. Not a broad ambition to “use AI in patient engagement.” A concrete workflow with repeat volume, clear handoffs, and measurable outcomes.
By August 2023, ClinicalTrials.gov listed 57 ongoing clinical trials using AI chatbots in healthcare, covering use cases such as medication education and adherence, vaccine hesitancy, sleep tracking, communicable-disease self-testing and reporting, mental health, and diabetic foot care, as documented by the U.S. National Library of Medicine overview on chatbots in healthcare. The same source notes a projected market expansion from US$196 million in 2022 to approximately US$1.2 billion by 2032. That combination matters. It shows these systems have moved beyond front-desk automation into longitudinal support and research-adjacent care processes.
Where chatbots create the most value
Some use cases are consistently stronger than others.
-
Access and navigation: Appointment booking, rescheduling, referrals, clinic directions, pre-visit instructions, insurance, or intake guidance.
-
Medication and adherence support: Refill reminders, education, follow-up check-ins, side-effect routing, pharmacy handoffs.
-
Post-discharge communication: Symptom check prompts, reminders about follow-up visits, care plan reinforcement, escalation to a nurse line when responses indicate risk.
-
Chronic care touchpoints: Ongoing support for diabetes, hypertension, sleep, and other recurring management needs.
-
Trial and program engagement: Enrollment guidance, reminder workflows, and structured patient follow-up for digital health studies or specialty programs.
These workflows create ROI because they sit at the intersection of volume and repeatability. Every time staff answer the same question, chase the same missed appointment, or manually route the same refill request, the organization is paying for process friction.
What good ROI actually looks like
In healthcare, ROI isn’t only financial. It often appears first in operational relief.
A patient support chatbot is worth funding when it does at least one of these well:
-
Reduces avoidable staff work: Front-desk and contact-center teams spend less time on repetitive queries.
-
Improves access: Patients can self-serve outside clinic hours.
-
Supports continuity: The system stays present between appointments.
-
Creates cleaner routing: The right issue reaches the right team faster.
-
Captures structured intent data: Product and operations teams learn what patients ask for most often.
Practical rule: If a use case doesn’t have a clear owner, an escalation path, and a measurable operational endpoint, it’s not ready for an AI chatbot.
The failure pattern is also predictable. Teams start with symptom triage, broad care advice, or open-ended generative interactions before they’ve solved scheduling, reminders, and authenticated account actions. That usually creates risk faster than value.
A stronger path is to sequence use cases by reliability. Start with high-frequency support tasks. Add transactional actions. Then expand toward higher-context care support only when governance, content control, and monitoring are already in place.
Navigating HIPAA Compliance and Data Privacy

A healthcare chatbot isn’t compliant because the cloud provider says the stack is HIPAA-eligible. That only means the platform can support a compliant implementation. The actual responsibility sits with the system design, vendor agreements, access model, data flows, and operating procedures.
Do this first
Start by classifying the chatbot by data exposure and action scope.
If the bot handles appointment questions without identifying a person, the risk profile is lower. If it authenticates a patient, accesses records, processes refill requests, or writes interaction data back into clinical systems, you’re in a different category. At that point, architecture and compliance can’t be separated.
The core controls usually include:
-
Protected Health Information boundaries: Define what PHI the bot can collect, display, store, or transmit.
-
Business Associate Agreements: Every relevant vendor in the chain needs the right contractual posture.
-
Encryption: Data needs protection in transit and at rest.
-
Access control: Limit who can view logs, transcripts, and linked patient context.
-
Auditability: Every meaningful action should be traceable.
-
Retention rules: Transcript storage and deletion policies must match organizational policy.
Do not rely on generic conversation logs
One of the most common implementation mistakes is logging too much data in too many places. Teams enable debugging, analytics, model tracing, prompt history, and chat transcript storage across multiple tools. Months later, nobody can clearly answer where sensitive data lives.
A safer pattern is to design for the minimum necessary data from the start.
-
Store only what operations need: Not every transcript belongs in long-term storage.
-
Separate observability from PHI: Technical telemetry shouldn’t automatically include patient identifiers.
-
Tokenize where possible: Internal references are often enough for system workflows.
-
Review vendor defaults: Many platforms log by default in ways healthcare teams shouldn’t accept blindly.
Compliance work gets easier when engineers map data movement before they write prompts.
Accessibility belongs in the same planning conversation. If the chatbot becomes a major front door for care support, the interface has to work for more than digitally fluent users. Teams working through that layer of design often benefit from practical guidance on digital accessibility in healthcare, especially around content clarity, assistive technology support, and inclusive interaction patterns.
What trust looks like in production
Patients don’t experience HIPAA as a policy document. They experience it as confidence that the system behaves predictably. The chatbot should disclose what it can do, what it can’t do, when a human is involved, and how sensitive information is handled.
That’s also where governance documents matter operationally, not just legally. Security reviews, incident response planning, role-based permissions, and clinical content approval all shape the product patients use. For teams formalizing these controls, an AI regulatory compliance and security framework for MedTech is a useful planning reference.
Core Technical Architecture and Key Integrations
A production chatbot is a system, not a model. The language layer gets most of the attention, but the integration layer creates most of the value.
Healthcare chatbots increasingly connect to EHRs, pharmacy systems, appointment platforms, patient portals, and wearables so they can answer questions and execute actions. Industry sources also cite that well-integrated chatbots can resolve up to 80% of repetitive, low-complexity inquiries without human involvement, according to Kayako’s analysis of AI chatbots for healthcare. That closed-loop workflow is the difference between an assistant that sounds helpful and one that reduces operational load.
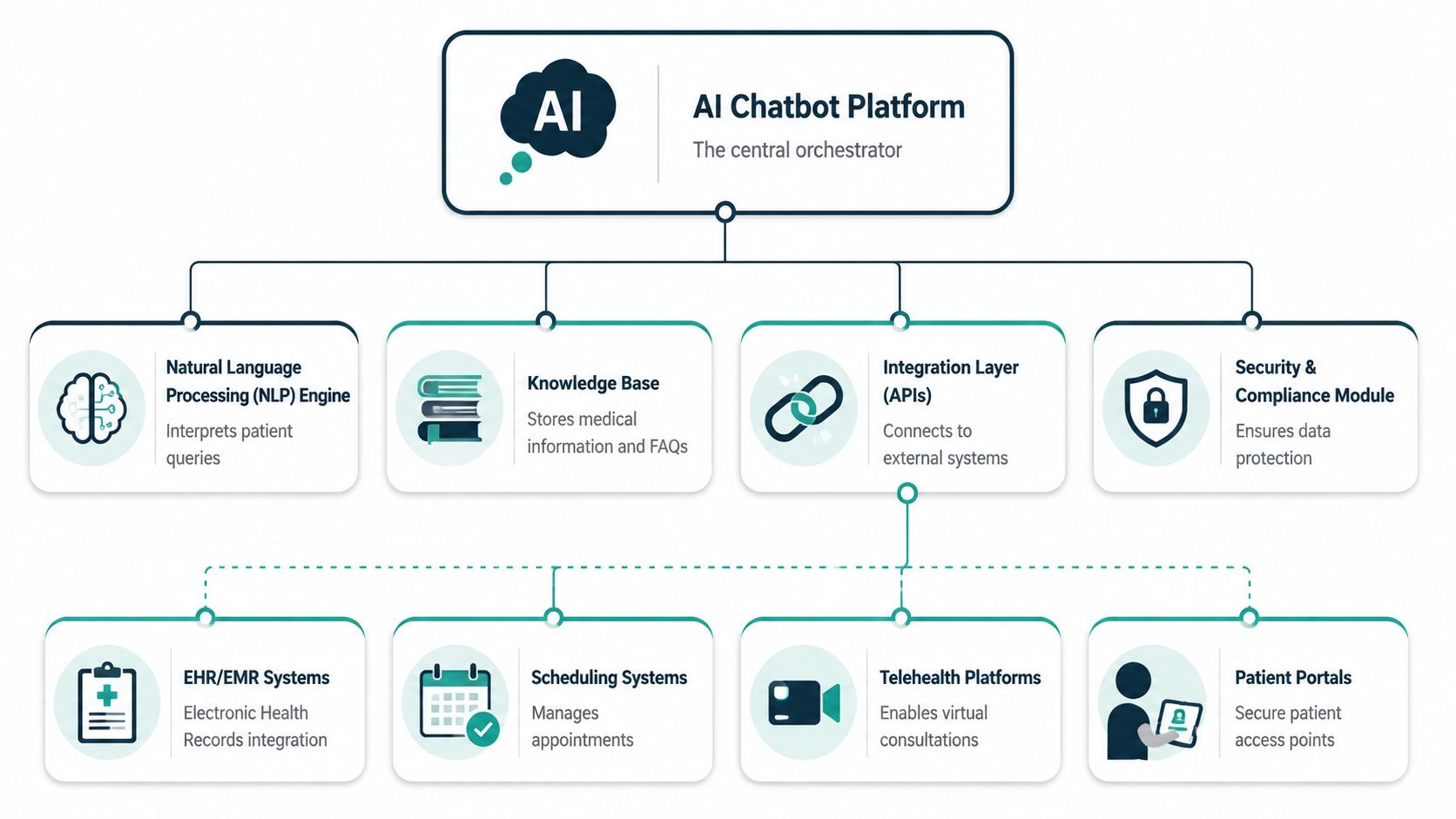
The core stack
Most well-developed implementations include five layers.
| Layer | What it does | Common design concern |
|---|---|---|
| Conversation layer | Handles chat UI, messaging flow, and channel delivery | Keeping interactions clear and bounded |
| Orchestration layer | Routes intents, applies rules, triggers tools, manages fallbacks | Preventing unsafe or ambiguous actions |
| Knowledge layer | Retrieves approved content, FAQs, care instructions, policy text | Source freshness and clinical review |
| Integration layer | Connects scheduling, EHR, portal, pharmacy, CRM, telehealth | Authentication, permissions, and data mapping |
| Security and monitoring layer | Logs events, enforces access control, supports audit and alerting | Avoiding sensitive over-logging |
Build versus configure
There isn't one right stack for every organization. Some teams use a conversational platform like Google Dialogflow or Microsoft Azure Bot Service for flow control, then add retrieval, orchestration, and custom APIs around it. Others build a more customized stack around an LLM gateway, a retrieval layer, and service-specific connectors.
The choice depends on constraints:
-
Use a platform-first approach when speed, standard channels, and predictable flows matter most.
-
Use a custom orchestration approach when you need deeper workflow logic, stronger guardrails, or tighter alignment with internal systems.
-
Use retrieval-augmented generation carefully when answers must come from approved healthcare content rather than model memory.
It becomes critical for healthcare integrations to stop being a technical afterthought and become the heart of the product. If the chatbot can't check appointment availability, submit a refill request, verify identity, or pull the right educational content for the right patient context, it won't hold up in production.
The integration details that usually break first
Teams often underestimate the non-LLM work. In most deployments, the difficult parts are identity, permissions, and workflow state.
Watch these closely:
-
Authentication and session continuity: A patient may begin anonymously, then need a secure login before taking action.
-
EHR interoperability: Read and write permissions are rarely simple. Not every field should be exposed conversationally.
-
Scheduling logic: Appointment types, provider rules, location constraints, and cancellation policies create edge cases fast.
-
Pharmacy workflows: Refill requests need routing logic, policy checks, and staff oversight.
-
Escalation infrastructure: Human handoff needs context transfer, not just a phone number.
If the bot can answer but not act, patients still end up calling staff.
For organizations building a broader patient-facing product, the architecture often overlaps with custom software development and even SaaS product development, especially when the chatbot sits inside a multi-tenant portal or member experience platform.
One implementation option in this space is Bridge Global's AI development services, which include healthcare chatbot system work such as scheduling, prescription renewal support, and integration-led patient workflows. That matters less as a brand point than as a reminder that healthcare chatbot delivery is usually an engineering and systems problem before it's a UX novelty.
Designing and Training Empathetic Conversations
The fastest way to lose trust is to build a chatbot that sounds polished but behaves carelessly. Patients don't need a witty assistant. They need one that is clear, calm, and safe.
A recent review in JMIR on healthcare chatbots and LLMs describes AI chatbots as increasingly used for remote health services, patient support, care management, and mental health support, with growing use in prevention, diagnosis, and treatment support. The same review frames them as support tools, not replacements for clinical judgment. That distinction should shape every conversation design decision.
What empathetic design looks like
Empathy in healthcare chatbots isn't about simulated emotion. It's about reducing confusion and showing appropriate restraint.
That usually means:
-
Use plain language: Short answers beat dense paragraphs.
-
Acknowledge uncertainty: If the system doesn't know, it should say so.
-
Guide the next step: “Book follow-up,” “call the clinic,” or “I can connect you to support” is more useful than generic reassurance.
-
Avoid overconfident phrasing: The bot shouldn't imply diagnosis or certainty where none exists.
-
Set role boundaries early: Patients should know whether they're using a scheduling assistant, support bot, or symptom guidance tool.
Training for accuracy, not just fluency
LLMs can generate persuasive text. That's not enough for patient support.
A safer training and response strategy usually includes:
-
Approved content sources
Use reviewed care instructions, medication guidance, program FAQs, and policy content. Don't let the model invent from open-ended prompts. -
Retrieval over memory
Pull answers from a controlled knowledge base when possible. In such instances, RAG becomes useful, especially for organization-specific content. -
De-identified training material
If conversation data is used to improve the system, remove unnecessary identifiers and govern access tightly. -
Human review loops
Product owners, compliance leads, and clinical stakeholders should review failed intents, risky outputs, and escalation transcripts regularly.
A good healthcare chatbot doesn't try to sound like a clinician. It helps patients get to the right information or person faster.
Escalation design is part of empathy, too. The bot should recognize distress, repeated misunderstanding, off-policy requests, and any situation where ambiguity becomes risky. The handoff has to preserve context. Otherwise, the patient has to repeat everything, and the chatbot becomes another barrier instead of a support layer.
Organizations that are building broader enterprise AI solutions often learn this lesson quickly. The hardest part isn't making the model talk. It's deciding when it shouldn't.
As we explored in our guide to broader AI product delivery, disciplined scope, approved content, and feedback loops usually outperform ambitious open-ended conversation design in regulated environments.
Measuring Success and Mitigating Common Pitfalls
A chatbot project shouldn't be judged by launch status. It should be judged by whether patients complete useful tasks safely and whether staff workload changes.
The evidence base also calls for caution. A JMIR AI review and case study on underserved populations found that among 103 studies, only 14.6% addressed triage, screening, risk assessment, and referral, and it emphasized that clinical effectiveness is still being established. That's the most important reality check in this space. Convenience features are easier to ship than equitable clinical value.
The metrics that matter
Usage counts alone don't tell you much. A better scorecard combines operational, experience, and safety indicators.
| Metric | Description | Example target |
|---|---|---|
| Task completion rate | How often patients finish the intended workflow | Improve steadily after launch |
| Containment rate | How often the chatbot resolves eligible low-complexity requests without staff intervention | Increase only where safety is preserved |
| Escalation quality | Whether handoffs happen at the right moment with sufficient context | Reduce failed or repeated handoffs |
| Patient satisfaction | How patients rate the interaction after completion | Track by use case, not only overall |
| Deflection impact | Whether support volume shifts away from repetitive channels | Validate against staffing and queue data |
| Content accuracy | Whether answers match approved source content | Maintain strict review thresholds |
| Accessibility performance | Whether patients across abilities and literacy levels can complete tasks | Improve through usability testing |
What fails in the real world
Several patterns appear again and again.
-
Overscoped first releases: Teams launch with symptom checking, care advice, scheduling, billing, and triage all at once.
-
Weak onboarding: Patients don’t understand what the chatbot can do, so they ask everything and trust drops quickly.
-
No segmentation: A workflow that works for digitally confident adults may fail for older adults or low-literacy populations.
-
Inadequate fallback design: The bot says “I’m sorry” repeatedly instead of moving the patient to a human path.
-
Shallow evaluation: Teams celebrate usage while ignoring completion failures or unsafe responses.
The underserved population evidence gap matters because it forces a more honest question: does the chatbot work for the patient population you serve? Not an average user in a product deck. Your patients, with your channels, your languages, your staffing model, and your access constraints.
Field note: A chatbot that performs well in demos can still underperform badly when trust, literacy, or device limitations enter the workflow.
Reviewing real client cases can help teams ask better questions. Not “Can AI do this?” but “What conditions make this implementation safe, useful, and supportable after launch?”
Your Implementation Roadmap to Get Started
Most failed chatbot projects don’t fail because the model was weak. They fail because the rollout sequence was wrong. Teams push toward a broad launch before they’ve validated scope, governance, and integrations.

A practical rollout pattern
-
Define one narrow use case
Start with a support workflow that has repeat volume and low ambiguity. Scheduling, reminders, and refill routing are usually better first bets than broad clinical advice. -
Design the operating model
Clarify content ownership, escalation rules, transcript handling, compliance review, and support-team responsibilities before development moves far. -
Build the integration path early
Connect the bot to the systems that matter most. In healthcare, value comes from action, not from conversation alone. -
Pilot before scale
Use a limited rollout to observe real patient behavior, staff handoffs, failed intents, and content gaps. -
Expand only after measured stability
Add new workflows when the first one is reliable, governable, and supportable.
What to line up internally
The strongest implementations usually align product, engineering, compliance, clinical review, and operations from the first workshop. If one of those groups enters late, redesign is almost guaranteed.
For organizations that want structure around this process, an AI implementation roadmap and clear software development service models can help frame delivery choices, ownership, and risk before build decisions lock in.
Frequently Asked Questions
Can an AI chatbot diagnose patients?
It shouldn’t be positioned as a diagnostic authority. In patient support, the safer role is guidance, navigation, information retrieval, and workflow execution under controlled rules. Clinical judgment still belongs to licensed professionals.
What’s the best first use case?
Choose a high-volume task with low ambiguity and clear escalation, such as scheduling, medication reminders, refill routing, or post-visit follow-up. Those workflows usually create value faster and with less risk.
Does a HIPAA-eligible platform make the chatbot compliant?
No. HIPAA eligibility only means the platform can be used in a compliant setup. The implementation still depends on your access controls, BAAs, auditability, data minimization, storage rules, and operating processes.
Should the chatbot use a general-purpose LLM?
Sometimes, but only with guardrails. In healthcare, model choice matters less than retrieval strategy, system prompts, approved content sources, action controls, and human escalation design.
How long does implementation take?
It depends on scope, integrations, compliance review, and whether you’re embedding the chatbot into an existing product. A narrow support workflow launches far faster than a multi-channel assistant connected to several clinical systems.
If you’re planning AI chatbots for patient support, Bridge Global can help evaluate scope, integration complexity, and compliance requirements before you commit to a build. The most successful projects start with a narrow operational target, a realistic architecture, and a delivery discipline that fits healthcare rather than generic AI product patterns.
About Upendra Jith
Upendrajith completed his Master's in English and has been a commercial content developer for the past three years. He's more inclined to develop content with a 'street-smart' delivery on topics such as technology, media, or anything he can get his hands on. He has a fixation on lyrics, dark poetry, media, technology, and flow arts.
View all posts by Upendra Jith →