


Healthcare Data Governance: A Guide for Healthtech Leaders
The numbers alone should change how leaders think about healthcare data governance. The healthcare industry spends more than $2 billion annually on provider data management, yet 49 percent of provider data contains inaccuracies or errors, according to LexisNexis Risk Solutions. That's not a paperwork problem. It's a product problem, a clinical risk problem, and a growth problem.
Often, teams still treat governance as a compliance layer that sits outside product delivery. In practice, it sits inside everything. It affects identity resolution, billing, audit readiness, interoperability, AI quality, access control, and how confidently teams can scale new features. If you're building regulated software, governance is the operating model that determines whether your data can be trusted when it matters.
What Is Healthcare Data Governance Really

Healthcare data governance sets the rules for how health data is defined, collected, corrected, shared, protected, and retired. It assigns ownership. It establishes approved sources. It defines who can change a field, who can see it, and what evidence exists when someone asks, “Why did this record change?”
That sounds administrative until a product team tries to reconcile patient identity across an EHR feed, claims data, CRM records, and analytics tables. At that point, governance becomes operating infrastructure. Without it, teams argue over which record is right, engineers hard-code exceptions, and compliance inherits cleanup work after the fact.
The spending and error rates cited earlier make the point. Healthcare does not struggle because teams lack tools. It struggles because many organizations still lack clear decision rights, shared definitions, and accountability for data quality.
Governance is a business system, not a paperwork exercise
In practice, healthcare data governance covers six decisions that affect daily operations:
-
who owns each critical dataset
-
which source is authoritative for each field
-
what quality thresholds trigger review or correction
-
how access is approved, logged, and revoked
-
how data moves between systems and vendors
-
how exceptions are documented and audited
If those decisions live only in Slack threads, tribal knowledge, or one experienced analyst's head, the organization does not have governance. It has dependency risk.
A sound program turns data into an asset the business can use with confidence. That matters for compliance, but it also matters for growth. Clean provider, patient, and operational data reduces rework in implementation, shortens customer onboarding, improves reporting accuracy, and lowers the cost of integrating new products, partners, and AI features.
Practical rule: If a team cannot name the owner of a critical dataset, identify the approved source, and show how changes are reviewed, governance is still informal.
The trade-off looks different for startups and enterprises
Startups usually avoid formal governance for understandable reasons. They need speed, they have small teams, and one person often covers product ops, implementation, and compliance. A lightweight model is usually the right call early on. But lightweight cannot mean undefined. Even at an early stage, teams need a data owner for core entities, a small set of approved definitions, access rules for sensitive data, and a clear process for correcting errors.
Enterprises face the opposite problem. Ownership exists on paper, but approval chains, duplicate controls, and overlapping committees slow down delivery. I see this often in health systems and larger vendors. The answer is not more policy. It is tighter scope, clearer stewardship, and controls attached to the highest-risk datasets first.
Both groups face the same economic question. What does poor data quality cost compared with the cost of prevention? In startups, the loss often shows up as implementation delays, customer distrust, and expensive rework during SOC 2, HIPAA, or payer diligence. In enterprises, it shows up as audit friction, denied claims, broken integrations, and labor spent reconciling systems that should agree by design.
If your environment includes M365, shared drives, or document-heavy workflows, governance has to cover collaboration tools too. Access sprawl often starts outside core clinical systems and then creates downstream risk. The controls in this guide to avoiding data exposure in M365 are relevant because healthcare incidents often begin with poorly governed documents, exports, and permissions long before they appear in an audit log.
The High Stakes of Getting Data Governance Wrong
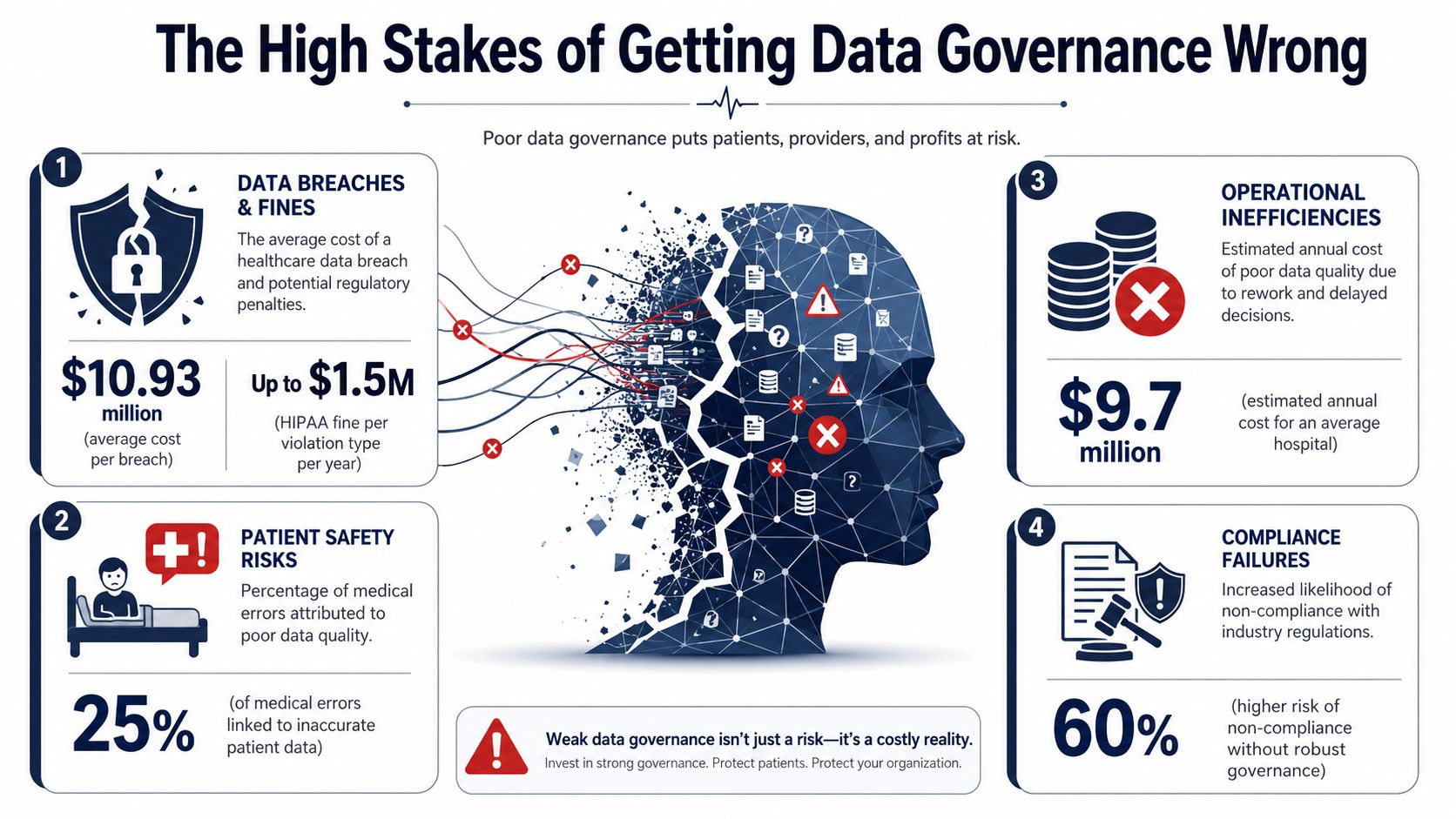
Analysts at Varonis report that 90 percent of healthcare organizations experience at least one security breach, with average costs reaching $10 million. For a startup, that can wipe out a funding round or stall a go-live with a key customer. For an enterprise, it can trigger audit scrutiny, contract disputes, and months of operational drag across security, legal, compliance, and revenue cycle teams.
Poor governance usually does not fail as a single headline event. It starts with ordinary control gaps. A role keeps access after a job change. An export includes fields no one approved. A billing rule runs against stale provider or payer data. Then an incident, audit, or implementation exposes the weakness.
HIPAA turns weak governance into operational pressure
Under HIPAA, organizations handling ePHI must establish breach notification procedures with a 60-day timeline for large breaches and conduct risk analyses across storage, transmission, and access, as described in this healthcare governance overview.
Those requirements create pressure in places many teams delay because the work feels administrative until something breaks:
-
Risk analysis: Teams need a repeatable method to identify where ePHI lives, how it moves, and which controls fail open.
-
Breach response: Teams need named owners, documented steps, and evidence trails that hold up under review.
-
Access governance: Teams need least-necessary access based on role, not a permissions model built from exceptions.
Weak governance often means incident response starts with basic discovery. That is expensive, slow, and hard to defend.
Costs extend beyond fines
The direct penalty is only one part of the equation. Poor governance also shows up in delayed implementations, failed security reviews, lower buyer confidence, rework during diligence, and manual reconciliation work that keeps growing as volume increases.
The trade-off is different by company stage. Startups often accept loose controls to ship faster, but that shortcut gets expensive when an enterprise prospect asks for audit logs, data lineage, retention rules, and evidence that sensitive data is segregated correctly. Enterprises usually have the opposite problem. They carry too many controls, but cannot prove which ones reduce risk versus which ones slow delivery and inflate operating cost.
That is why governance deserves budget as a growth function, not just a compliance function. If better controls reduce implementation delays, shorten diligence cycles, prevent claims or billing errors, and avoid post-incident cleanup, the return is measurable in revenue protection and lower operating cost.
There is also a technical debt angle. Many governance failures trace back to legacy interfaces, fragmented identity, and partial cloud migrations. Teams modernizing older platforms should treat governance design and platform design as one workstream. Modernization Intel's cloud modernization guide is a useful reference here because cloud migration without data ownership, access controls, and lineage usually moves the risk rather than reducing it.
What usually fails first
The earliest failure points are rarely complex.
| Failure area | What it looks like in practice |
|---|---|
| Access control | Shared permissions, role creep, unclear approval paths |
| Data quality | Duplicate entities, stale provider records, inconsistent field formats |
| Auditability | Missing logs, undocumented transformations, weak lineage |
| Operational ownership | Engineering thinks compliance owns it, compliance thinks engineering owns it |
These issues have a direct business effect. Sales cycles slow down when security questionnaires expose gaps. Implementation teams spend time validating feeds that should already be governed. Finance absorbs avoidable leakage when bad reference data affects claims, billing, or reporting.
A governance program that works in healthcare reduces those losses while making the business easier to scale.
Building Your Healthcare Data Governance Framework
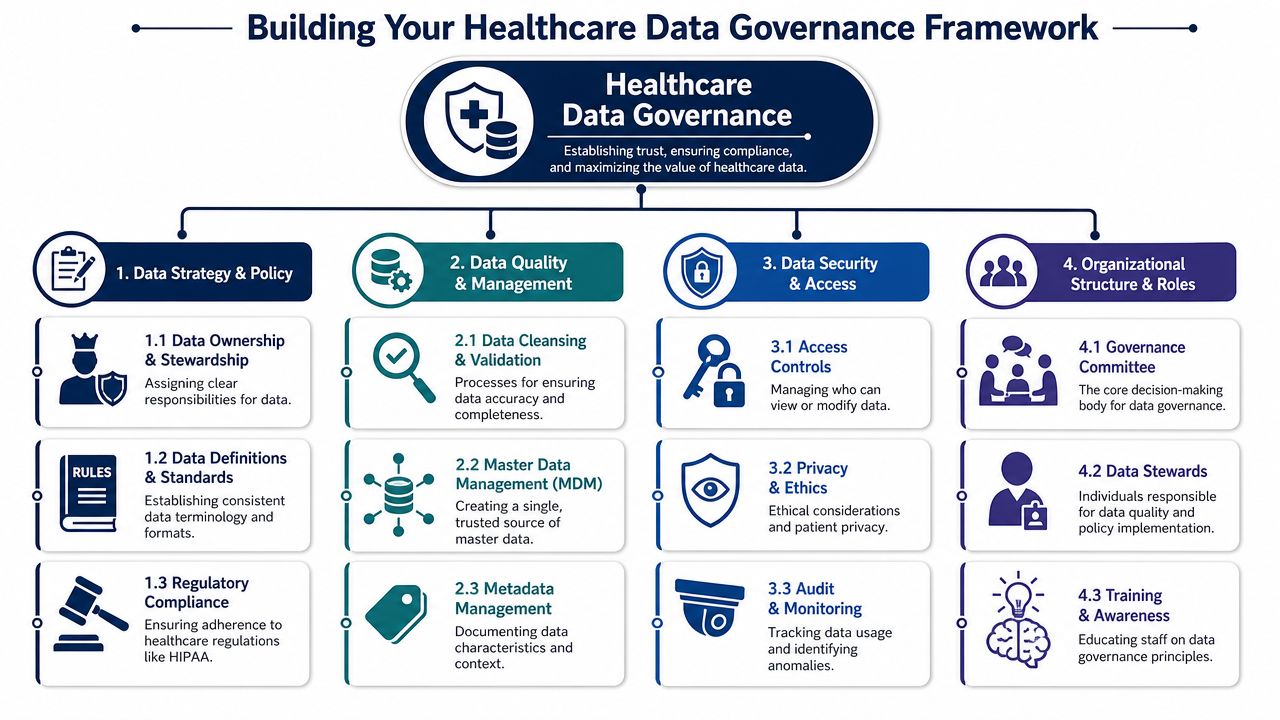
A healthcare data governance framework should answer a simple operational question. Who is allowed to do what with which data, under which rules, and how do you prove it later? If the framework cannot answer that quickly, it will fail under audit pressure, customer diligence, or scaling stress.
The right design depends on company stage. A startup usually needs a lighter control model that protects PHI, supports contracts, and keeps product delivery moving. An enterprise needs the same basics, but with stronger cross-system consistency, formal approvals, and traceability across business units, vendors, and acquired platforms. Both are solving for risk reduction and growth. The difference is how much process the business can afford before it starts slowing itself down.
Start with policy, scope, and decision rights
Policy should settle practical disputes before they become engineering rework or compliance findings. Define the system of record for patient identity, consent, provider data, encounter data, and billing data. Set retention rules for production records, exports, logs, backups, and training datasets. Specify which data classes need tighter approval, monitoring, or masking.
Decision rights matter just as much. If nobody can approve a new sensitive field, teams create workarounds. If too many people can approve it, standards drift. The fix is a short, written model that names who decides, who implements, and who signs off.
A useful starting structure looks like this:
-
Prioritize critical datasets: Patient, provider, location, encounter, claims, billing, and consent data usually create the highest operational and regulatory exposure.
-
Assign a business owner to each dataset: Ownership belongs with the function accountable for data quality, permitted use, and downstream impact.
-
Approve standard definitions: Terms such as “active patient,” “rendering provider,” or “clean claim” need one definition that reporting, product, and operations all use.
-
Document escalation paths: Teams need a clear route for exceptions, disputed definitions, and urgent access decisions.
Build controls into delivery, not cleanup
Governance breaks when teams treat quality and compliance as a review step at the end of delivery. Controls need to sit inside product requirements, schema design, ETL logic, API contracts, and internal admin tools.
That means validation at ingestion, clear field constraints, standardized code sets where they apply, and visible exception handling. It also means auditability by default. Critical writes should be attributable. Transformations should be documented. Access to sensitive workflows should leave a usable log trail.
I have seen startups postpone this because it feels faster to clean data later. The cost shows up in implementation delays, failed reporting, payer disputes, and expensive remediation when enterprise customers ask basic governance questions. Teams planning a platform refresh or integration cleanup should align governance with architecture decisions early. Healthcare data modernization planning is usually the point where ownership, lineage, and control gaps become obvious.
Strong governance lowers operating cost by preventing bad data from spreading into claims, reporting, support workflows, and customer implementations.
Secure access around real work patterns
Access design fails in two common ways. One model grants broad permissions because restricting access is inconvenient. The other model is so rigid that staff start using exports, screenshots, and informal workarounds.
Good governance defines access around actual job functions and sensitive actions, not generic department labels. Clinicians, billing staff, support teams, analysts, implementation specialists, and engineers do not need the same view of the same record. Some roles need full access to treatment data. Others need limited access to demographics, status, or operational metadata.
Use the framework to define:
-
Role-based access boundaries by workflow
-
Approval paths for privileged or time-bound access
-
Logging rules for viewing, editing, exporting, and deleting sensitive data
-
Minimum necessary standards for non-clinical users
-
De-identification and minimization rules for analytics, testing, and product review
Treat metadata as an operating asset
Metadata is what makes a governance program usable. Without it, teams cannot answer basic audit and incident questions with confidence. Where did this field originate? Which service changed it? Which reports depend on it? Which policy applies to it?
A practical metadata layer includes data dictionaries, sensitivity classification, lineage for high-risk flows, and mappings between business terms and technical schemas. Enterprises often buy tooling before they agree on naming and ownership. Startups often skip metadata until customer requirements force it. Both approaches create drag. Start with the datasets that drive revenue, compliance exposure, and operational reporting.
Create named accountability
Committees do not own data. People do.
The framework needs named roles with authority to make decisions and enough proximity to operations to spot issues early.
Key Data Governance Roles and Responsibilities
| Role | Primary Responsibility |
|---|---|
| Executive sponsor | Sets direction, resolves cross-functional conflicts, funds the program |
| Data owner | Approves definitions, access rules, and acceptable use for a dataset |
| Data steward | Maintains quality, supports policy execution, manages issue resolution |
| Security lead | Aligns governance controls with security and privacy requirements |
| Compliance lead | Interprets regulatory obligations and validates control coverage |
| Engineering lead | Implements controls in systems, pipelines, and application workflows |
| Product manager | Ensures governance requirements are reflected in product decisions and delivery scope |
What holds up in practice
Patterns are consistent across teams that make governance work.
-
What works: Small governance councils with decision authority, limited scope at launch, and measurable controls tied to high-risk datasets.
-
What works: Definitions, access rules, and retention requirements reviewed before new integrations or customer implementations go live.
-
What works: Exception handling that is documented, time-bound, and visible to compliance, security, and engineering.
-
What fails: Large policy libraries that nobody uses in delivery.
-
What fails: Ownership assigned to a shared mailbox, a committee, or “the data team.”
-
What fails: Governance that starts after systems are already live, customers are onboarded, and terminology conflicts are embedded across products.
The best frameworks do more than satisfy auditors. They shorten enterprise diligence, reduce rework, improve reporting accuracy, and give leadership a clearer view of operational risk. That is why governance belongs in the growth model, not just the compliance program.
Governance in the Age of AI and Interoperability
AI increases the cost of weak data. It doesn't hide it. If a model is trained on inconsistent records, ambiguous definitions, or poorly mapped exchanges, the output inherits those defects and can scale them faster than any manual workflow.
That's why governance has become a precondition for trustworthy AI development services. Before teams talk about copilots, prediction layers, or workflow automation, they need to know whether the source data is complete, traceable, permissioned, and semantically consistent.
Interoperability standards are governance tools
Standards like HL7, FHIR, and LOINC are often discussed as technical integration concerns. In reality, they're governance mechanisms because they preserve meaning across system boundaries. According to West Coast Consulting Group, adopting these standards directly reduces data structuring errors and semantic loss during exchange, and organizations that track KPIs such as data error rates and audit readiness scores see measurable improvements when governance committees mandate them.
That matters in every environment where records move between EHRs, scheduling systems, payer platforms, labs, and analytics layers. If one system treats a field as free text and another treats it as coded clinical data, your problem isn't only interoperability. It's governance failure expressed through interoperability.
AI needs lineage, controls, and limits
The most common mistake in AI programs is jumping from available data to model experimentation without documenting provenance and fitness for use. In healthcare, teams need stronger discipline.
A reliable AI-ready governance posture includes:
-
Lineage: You should be able to trace where training and inference data came from.
-
Access control: Sensitive datasets used for modeling need explicit approval paths.
-
Definition control: Feature engineering should rely on approved business terms, not analyst-specific shortcuts.
-
Use-case boundaries: Not every dataset that can be used should be used.
For product teams building healthcare integrations and larger enterprise AI solutions, this becomes a design discipline, not a review checkbox. The more systems connected, the more semantic drift can accumulate unless governance actively constrains it.
As we explored in our guide to healthcare data modernization, modernization only improves outcomes when the target architecture carries forward trusted definitions, control points, and clear ownership.
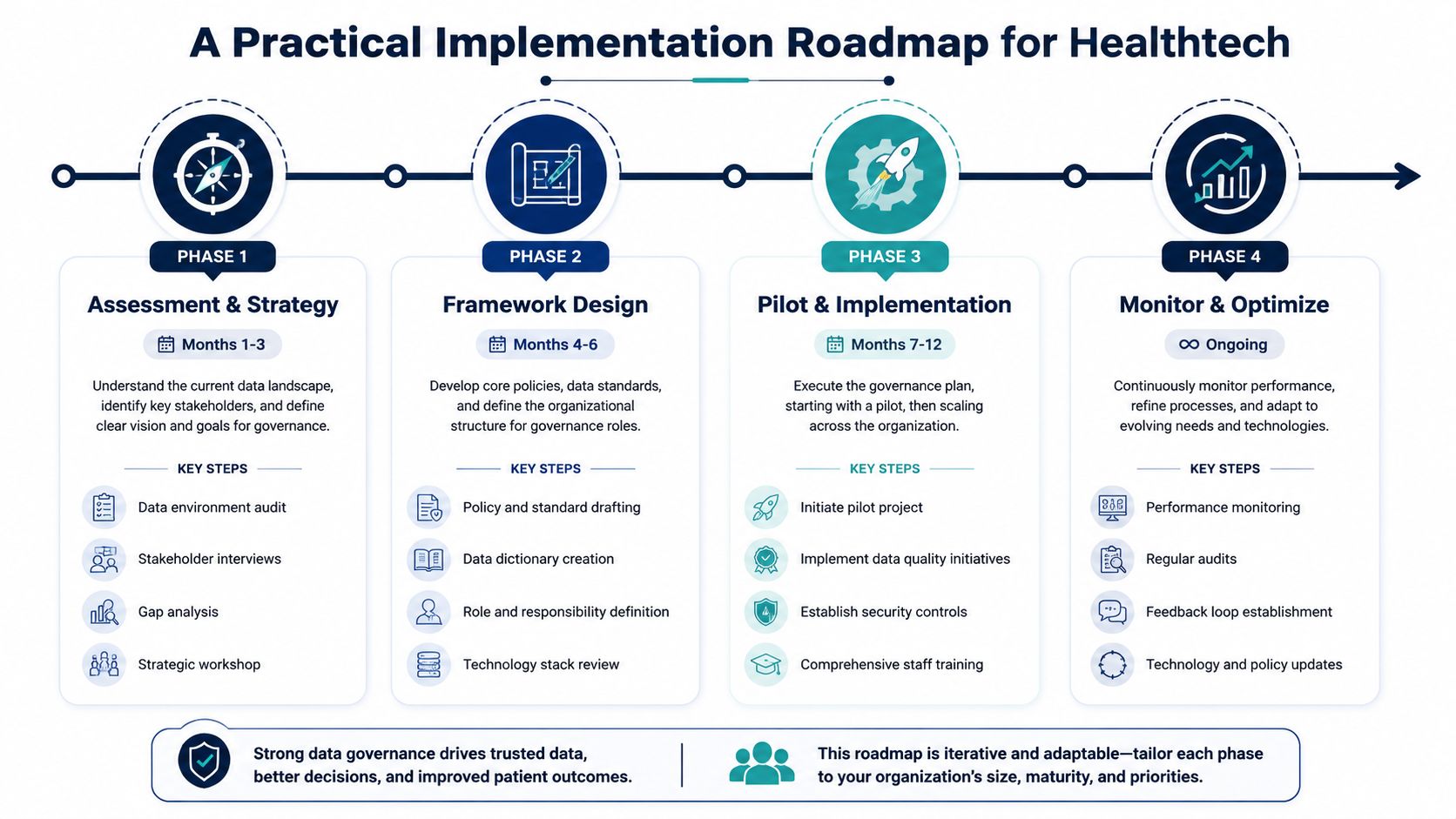
A Practical Implementation Roadmap for Healthtech
Most healthcare data governance programs fail because they start too wide. Leaders try to govern everything at once, create a large committee structure, and then discover no one has enough clarity to ship controls into real systems. A better path is phased, scoped, and tied to business friction.
The ROI case helps. Organizations with mature governance programs see 30% fewer data errors in patient records and 25% faster billing accuracy, according to Arcadia. That's the argument executives understand. Governance reduces operational drag, not just audit anxiety.
Phase 1: Assessment and business case
Start by mapping the systems and workflows that create the most downstream pain. For a startup, that might be patient identity, claims-related data, or customer-specific integrations. For an enterprise, it might be provider master data, consent handling, or cross-platform reporting.
Focus on a few questions:
-
Where does bad data trigger manual rework?
-
Which datasets appear in customer escalations, audit findings, or billing disputes?
-
Where is ownership unclear across product, engineering, compliance, and operations?
A startup should keep this lightweight. A founder, CTO, product lead, and compliance stakeholder can usually define an initial scope quickly. Enterprises need more coordination, but they still benefit from narrowing the first wave.
Phase 2: Design the minimum viable framework
The program takes on tangible form through these actions. Write only the policies you can enforce. Define only the standards you can test. Assign only the roles people will perform.
A minimum viable framework usually includes:
| Capability | Startup approach | Enterprise approach |
|---|---|---|
| Governance body | Small decision group | Formal council with cross-functional representation |
| Dataset scope | One or two critical domains | Prioritized domain rollout |
| Controls | Basic access, validation, audit logs | Layered controls, lineage, policy libraries |
| Documentation | Lean data dictionary and owners | Managed glossary, metadata catalog, control mapping |
This is also the point where delivery choices matter. Your governance plan should fit the way your product gets built. Teams should align implementation with suitable software development service models, especially when internal capacity is split across product delivery, compliance work, and customer commitments.
Phase 3: Pilot in one live workflow
Pick a workflow where quality and control problems are visible. Good pilots include provider onboarding, claims ingestion, referral routing, or customer reporting feeds. Avoid pilots that are politically easy but operationally irrelevant.
Choose a pilot where failure already costs time. That makes governance value obvious.
The pilot should include real control points: validation, ownership, access review, exception handling, and a small KPI set. For architecture teams refining this layer, our guide to healthcare data pipeline architecture is a useful companion because governance becomes enforceable only when it's built into the pipeline, not layered on after delivery.
Phase 4: Operationalize and extend
Once the first workflow stabilizes, extend by pattern, not by enthusiasm. Reuse the same governance artifacts where possible: owner templates, field classification rules, access approval flows, and issue triage processes.
This is also where AI enters carefully. If your roadmap includes autonomous or semi-autonomous decision support, the control model has to expand. Teams thinking ahead on that front may benefit from practical guidance on governing agentic AI systems, because governance gets harder when systems begin acting on data, not just analyzing it.
For healthtech companies building subscription platforms, governance should also be part of the release discipline for SaaS product development. New tenants, new integrations, and new analytics features all create opportunities for data drift unless governance evolves with the product.
An effective rollout often resembles a structured AI implementation roadmap. The sequence matters. Assessment first. Controlled design second. Pilot third. Continuous refinement after that.
From Compliance Burden to Strategic Advantage
The strongest teams stop framing healthcare data governance as overhead. They treat it as an asset that improves execution. Clean ownership reduces decision delays. Strong definitions improve integrations. Better controls improve trust with customers, partners, and regulators.
That's especially important for organizations scaling complex products. Governance supports cleaner releases, more defensible audits, and more reliable analytics. It also makes AI and interoperability initiatives more credible because the underlying data isn't a black box.
There's a direct relationship between trust in data and speed of delivery. Teams move faster when they don't have to debate which source is correct, manually reconcile records, or clean up preventable exceptions every sprint.
As we explored in our guide to HIPAA-compliant software development, compliance works best when it's built into architecture and delivery decisions from the start. Governance follows the same rule. It should shape how systems are modeled, connected, tested, and operated.
The organizations that benefit most don't build the biggest governance programs. They build the clearest ones. If you want to see how that kind of disciplined delivery shows up in real projects, reviewing strong client cases is often more useful than reading another abstract policy template. Mature execution is visible in systems that are auditable, scalable, and usable.
FAQs About Healthcare Data Governance
Healthcare leaders usually agree governance matters. The practical questions start once they try to implement it. The table below addresses the issues that come up most often in product, engineering, and operations reviews.
Frequently Asked Questions
| Question | Answer |
|---|---|
| Where should a startup begin with healthcare data governance? | Start with one critical data domain and one live workflow. Patient identity, provider data, billing-related records, or consent data are common candidates. Name an owner, define the source of truth, document access rules, and add validation where data enters the system. |
| Who should own healthcare data governance? | One team can't own it alone. Executive leadership should sponsor it. Business owners should own critical datasets. Engineering should implement controls in applications and pipelines. Compliance and security should define and validate control expectations. |
| What's the difference between data management and data governance? | Data management is the operational handling of data through storage, movement, transformation, and use. Governance sets the rules for how that management should happen, who makes decisions, and how quality, access, and compliance are enforced. |
| How often should governance policies be reviewed? | Review cadence should match regulatory exposure, release frequency, and system change volume. In practice, teams review policies whenever major workflows, integrations, or data uses change, and they add periodic reviews to avoid stale controls. |
| Do small healthtech companies need formal governance committees? | Not always. Early-stage companies usually need a small decision group rather than a large council. The key is decision authority, not ceremony. If the right people can approve standards, resolve ownership questions, and enforce controls, the structure is working. |
| Which metrics prove governance is working? | Use metrics tied to operational pain. Data error rates, billing accuracy, audit readiness, access review completion, issue resolution time, and time-to-access critical records are practical indicators. Avoid vanity dashboards that look complete but don't affect delivery or risk. |
| How does governance affect AI projects? | It determines whether AI can be trusted. Teams need lineage, approved data definitions, access controls, and clear use-case boundaries before they rely on models in sensitive workflows. Without that, AI scales uncertainty. |
| What's the most common implementation mistake? | Trying to govern every dataset at once. Teams get better results by starting narrow, proving value in one workflow, and extending a repeatable pattern across other domains. |
If you’re looking for a healthtech software development partner that understands compliant architecture, AI-enabled delivery, and scalable product engineering, Bridge Global can help. Its work spans custom healthcare software development, custom software development, and practical delivery models that support regulated growth.
About Preethi Saro Philip
Preethi Saro Philip is a Post Graduate Research Degree holder in Economics with more than 10 years of experience in writing, editing, research and teaching. She has an intense passion for content crafting and calls herself a ‘wordsmith’. She enjoys writing on wide-ranging topics including business, technology, health & lifestyle, education, environment etc.
View all posts by Preethi Saro Philip →