


Next-Generation Healthcare Platforms: A CTO’s Guide
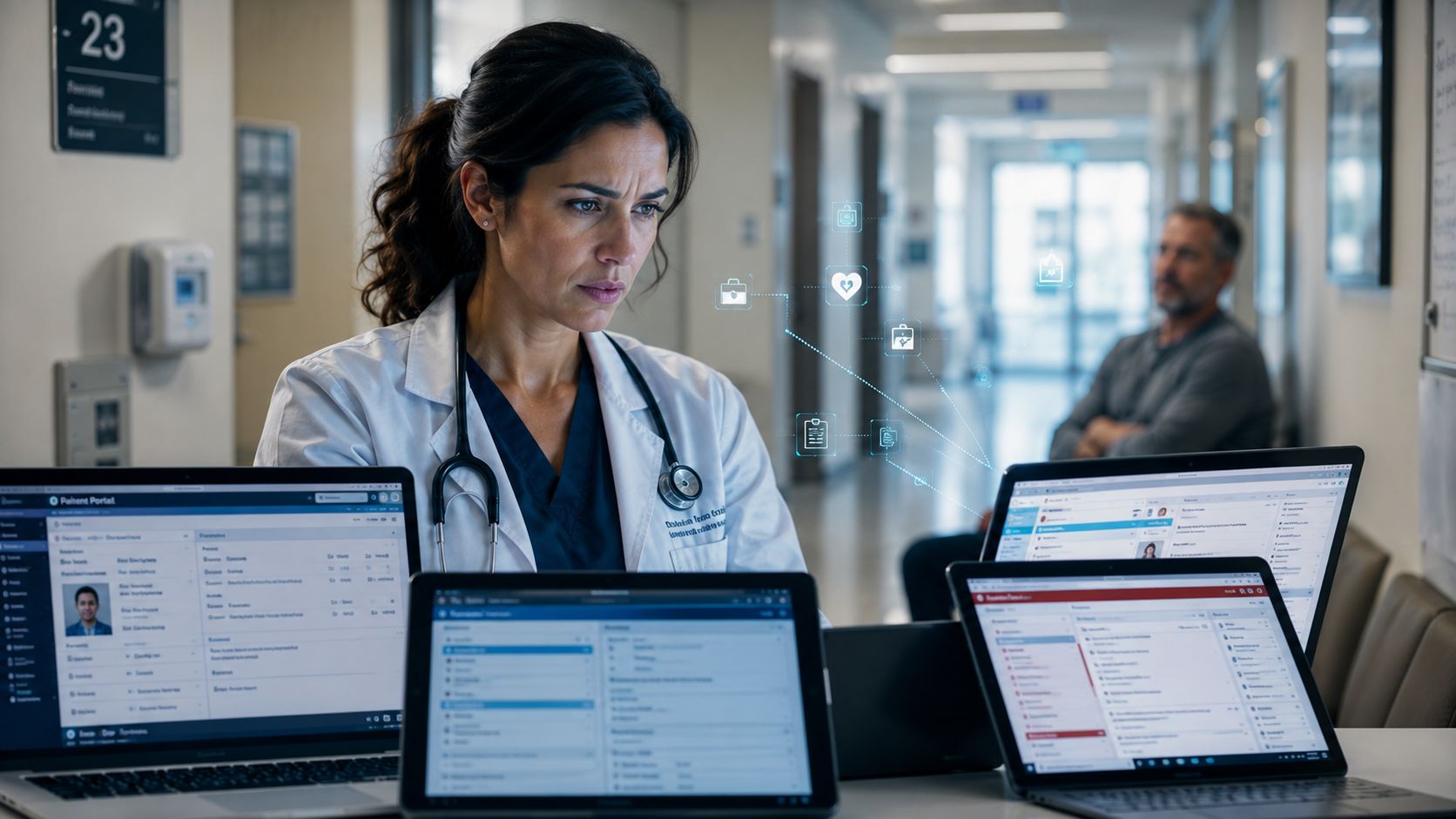
A provider executive sees the same failure pattern every week. A clinician opens one system for charting, another for scheduling, a separate portal for imaging, a billing screen that doesn't match the clinical record, and an inbox full of messages that never made it into the patient timeline. The patient experiences it as repetition, delay, and inconsistency. The team experiences it as friction and risk.
That's the operational mess next-generation healthcare platforms are meant to replace.
This isn't just an EHR refresh. It's a shift from isolated systems of record to connected systems of action. The organizations getting this right are building platforms that unify data, support decisions in the workflow, and give patients a digital experience that feels coherent instead of improvised. For startups, that often means choosing a narrow workflow and designing for interoperability from day one. For health systems, it means treating platform architecture as a strategic capability rather than an IT procurement exercise.
According to PwC's 2025 Future of Providers survey, healthcare is projected to be reengineered by 2035, driven by decentralized services and digital platforms powered by AI. The shift is already visible, with over 40% of Gen Z and millennials in the survey reporting that they've used virtual visits. That's a signal. Care is moving outside the hospital's four walls, and platform design has to follow.
A modern build starts with the right healthtech software development partner. The hard part isn't writing code. It's making architecture, compliance, data models, and adoption work together under real clinical constraints.
Introduction: The End of Disconnected Healthcare
A fragmented healthcare stack breaks trust long before it breaks compliance. The symptoms are easy to spot. Duplicate patient records. Manual prior authorization workarounds. Care teams copying information across tabs because the systems in front of them don't speak the same language.
What replaces that mess isn't a single magic product. It's a platform approach that treats patient identity, consent, clinical context, communication, and analytics as shared capabilities instead of isolated modules. That distinction matters. Teams that keep buying point solutions usually add another layer of complexity. Teams that design around a platform create a base they can keep extending.
Why the old model is breaking
Legacy environments were built around documentation and billing. Those functions still matter, but they're no longer enough. Care now spans virtual visits, remote monitoring, patient messaging, home-based workflows, device data, and third-party services. A system built mainly to store transactions can't easily orchestrate all of that.
Three pressures are pushing leaders to rethink the stack:
Care is becoming distributed: Patients expect interactions across mobile, virtual, and in-person channels.
Clinical decisions need context: Raw records aren't enough when teams need timely, usable information at the point of care.
Operations need flexibility: New service lines, partnerships, and reimbursement models demand systems that can adapt without a full rebuild.
Practical rule: If your architecture makes every new workflow feel like a special exception, you don't have a platform. You have an accumulation of software.
What survival looks like now
The strongest healthcare organizations are turning hospitals and health systems into anchors for broader care networks, while digital tools support prevention, monitoring, and coordination across settings, as described in the earlier PwC projection. That changes what leaders need to fund. The priority shifts from buying features to creating durable capabilities.
For startups, this creates an opening. You don't need to outbuild a large EHR vendor feature for feature. You need to solve a painful workflow, connect cleanly to the surrounding ecosystem, and make the user experience meaningfully better. For incumbents, the lesson is less comfortable. Incremental patching won't keep up with patient expectations or clinician workload.
Defining Next-Generation Healthcare Platforms
A useful way to think about this shift is the move from feature phones to smartphones. A traditional EHR is often a tightly controlled system optimized for recordkeeping. A next-generation platform is an extensible environment where records, workflows, intelligence, and external services work together.
That doesn't mean the EHR disappears. It means the EHR stops being the whole strategy.
The practical definition
In operational terms, next-generation healthcare platforms prioritize data fluidity over data capture, proactive insight over passive storage, and open ecosystems over closed applications. They support clinical and administrative workflows, but they're also designed to ingest device data, expose APIs, manage consent, trigger automation, and deliver intelligence inside the workflow.
If your team is planning custom healthcare software development, that distinction should shape every early decision. Data models, service boundaries, user roles, audit design, and integration patterns all look different when you're building a platform instead of a single-purpose application.
For teams sorting through interoperability constraints, we explored some of the implementation friction in our guide to healthcare data interoperability challenges.
Traditional EHR vs. Next-Generation Platform
| Aspect | Traditional EHR | Next-Generation Platform |
|---|---|---|
| Data model | Focused on internal records and transactions | Designed to combine clinical, operational, patient-generated, and partner data |
| Interoperability | Limited or vendor-controlled interfaces | API-first design with FHIR, HL7, and extensible connectors |
| Intelligence | Reactive documentation support | Embedded analytics, decision support, and AI-assisted workflows |
| User experience | Staff-centered and often workflow-rigid | Role-based experiences for clinicians, staff, patients, and partners |
| Scalability | Expansion often requires customization inside the core system | Modular services can evolve independently |
| Ecosystem | Closed or difficult to extend | Open to apps, devices, and external services |
The architectural mindset that changes the outcome
The teams that succeed here stop asking, “Which system should own everything?” and start asking, “Which capabilities should be shared across the ecosystem?” That usually leads to a service-based architecture with identity, consent, messaging, scheduling, and data access abstracted away from any one front end.
If you're evaluating the infrastructure side of that transition, this primer on the future of cloud native architecture is a useful companion because it explains why resilience, portability, and service decomposition matter when healthcare workloads start expanding across channels and partners.
A next-generation platform doesn't win because it stores more data. It wins because clinicians and patients can actually use that data in time to change an outcome.
The Four Pillars of a Modern Healthcare Platform
A founder gets a pilot signed with a regional health system, then discovers the actual work starts after the contract. One clinic still sends HL7 v2 messages through an aging interface engine. Another expects FHIR APIs. Rural patients lose video connections halfway through visits. The compliance officer asks how consent is enforced when data crosses partners. These are the conditions that expose whether a platform has been engineered for healthcare or just adapted to it.
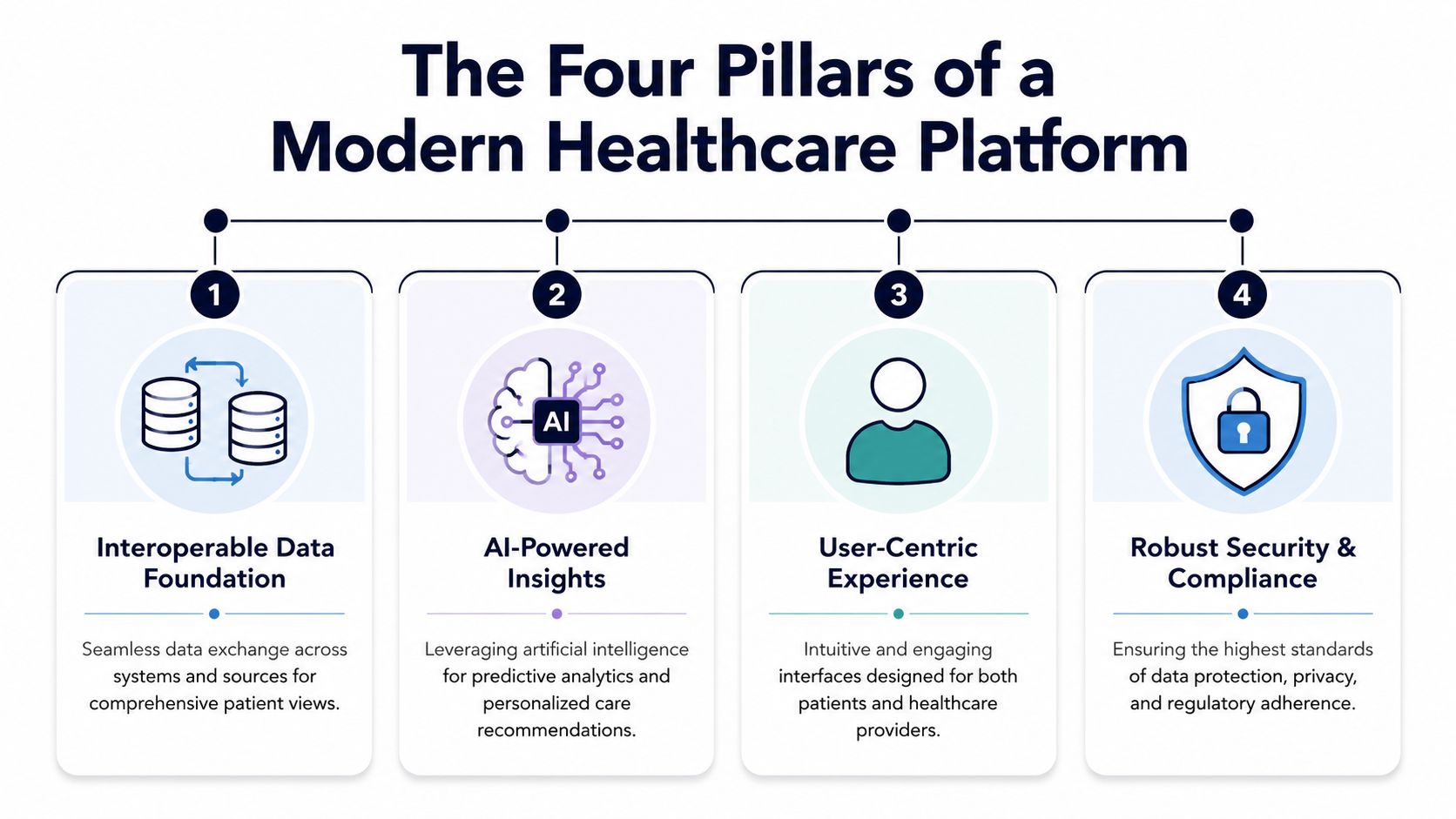
Interoperable data foundation
The first pillar is a data foundation that can produce a trustworthy patient record under real operating conditions. Supporting FHIR is only part of the job. Teams also need identity resolution, terminology management, source ranking, event processing, and a clear policy for what happens when records conflict.
The practical mistake is trying to normalize everything on day one. A better approach is to map the workflows where bad or late data creates the highest clinical or operational risk. Admission notifications, medication history, lab results, scheduling changes, and referral status usually rise to the top. That is where healthcare integrations stop being back-office plumbing and start affecting care quality, reimbursement, and staff workload.
A usable foundation usually includes:
Canonical data models: So downstream teams work from shared definitions instead of translating the same payload in different ways.
Event-driven exchange: So a discharge, critical result, or missed appointment can trigger the next action quickly.
Governed APIs: So partner access, app extensions, and internal product teams can build without creating policy drift.
Offline and low-bandwidth tolerance: So clinics in underserved areas are not excluded by an architecture that assumes constant high-quality connectivity.
AI-powered insights
The second pillar is applied AI, but only where teams can validate safety, fairness, and operational value. In healthcare, an impressive demo is easy. A model that holds up across specialties, languages, documentation styles, and uneven data quality is much harder.
The strongest early use cases sit close to workflow. Documentation support, summarization, chart review, triage assistance, and operational forecasting can reduce administrative load when the output is auditable and easy to override. According to IDC's analysis of next-generation EHR features, embedded analytics and generative AI can improve workflows, support safer and more personalized care, and improve operations when integrated into clinical systems rather than deployed as a separate novelty.
There is also a market example with a clear operational outcome. Clinicians using automated conversation-to-SOAP-note transformation in NextGen Clinical AI can save up to 2.5 hours per day, according to NextGen Healthcare.
That kind of result gets attention, but implementation discipline decides whether AI keeps that value in production. Teams need model monitoring, human review paths, fallback behavior, and bias testing across age, language, geography, and socioeconomic context. If training data underrepresents rural populations or minority communities, the product can widen care gaps while appearing statistically sound in aggregate. As noted earlier, AI development capability matters less than governance, validation, and adoption inside the workflow.
User-centric experience
The third pillar is experience design grounded in real care delivery. Poor UX in healthcare does more than frustrate users. It slows visits, hides context, encourages workarounds, and reduces data quality.
Different users need different products, not one crowded interface with role flags. Clinicians need fast context and fewer clicks. Operations teams need queues, exceptions, and handoff visibility. Patients need mobile-friendly flows, plain language, and communication options that match their circumstances. That last point matters more than many teams admit. A platform built for always-on broadband, long forms, and high health literacy will fail part of the population it claims to serve.
RxPx describes the patient engagement side well: the platform has to connect with provider portals and electronic medical records while supporting clear communication among providers, care teams, and patients. I would add one more standard from implementation experience. If a patient in a low-connectivity area cannot complete the key task over a basic mobile connection, the design is not finished.
Security and compliance architecture
The fourth pillar is security and compliance built into the platform model itself. Access control, consent, auditability, encryption, retention, and policy enforcement belong in the core services layer, not in scattered application logic.
Technical trade-offs become executive decisions. Fine-grained access control improves safety, but it can slow delivery if the policy model is too complex too early. Centralized consent enforcement improves consistency, but only if every app and integration uses it. Detailed audit logs support investigations and regulatory reviews, but they also increase storage, operational overhead, and data governance obligations.
The patterns that hold up over time are well understood:
Role-based and attribute-aware access: Baseline permissions plus contextual rules for cases such as cross-organization care teams or delegated access.
Consent as a shared service: A single enforcement point is easier to test, update, and audit than duplicated logic in front-end applications.
Audit trails by default: Sensitive actions should be traceable without custom work each time a new feature ships.
Data residency planning: Cross-border deployments, sovereign cloud requirements, and regional health data rules need to be addressed before expansion, not after it.
Founders sometimes treat this pillar as a late-stage hardening exercise. It is an architectural choice from the start. If the first three pillars create access, intelligence, and engagement, this one determines whether the platform can be trusted with real care delivery at scale.
Reference Architecture and Technology Stack
CTOs usually get in trouble when they copy an architecture diagram from a conference slide and assume it's a blueprint. A working healthcare platform needs modularity, but it also needs restraint. Too much early complexity creates operational drag before the product has proven value.
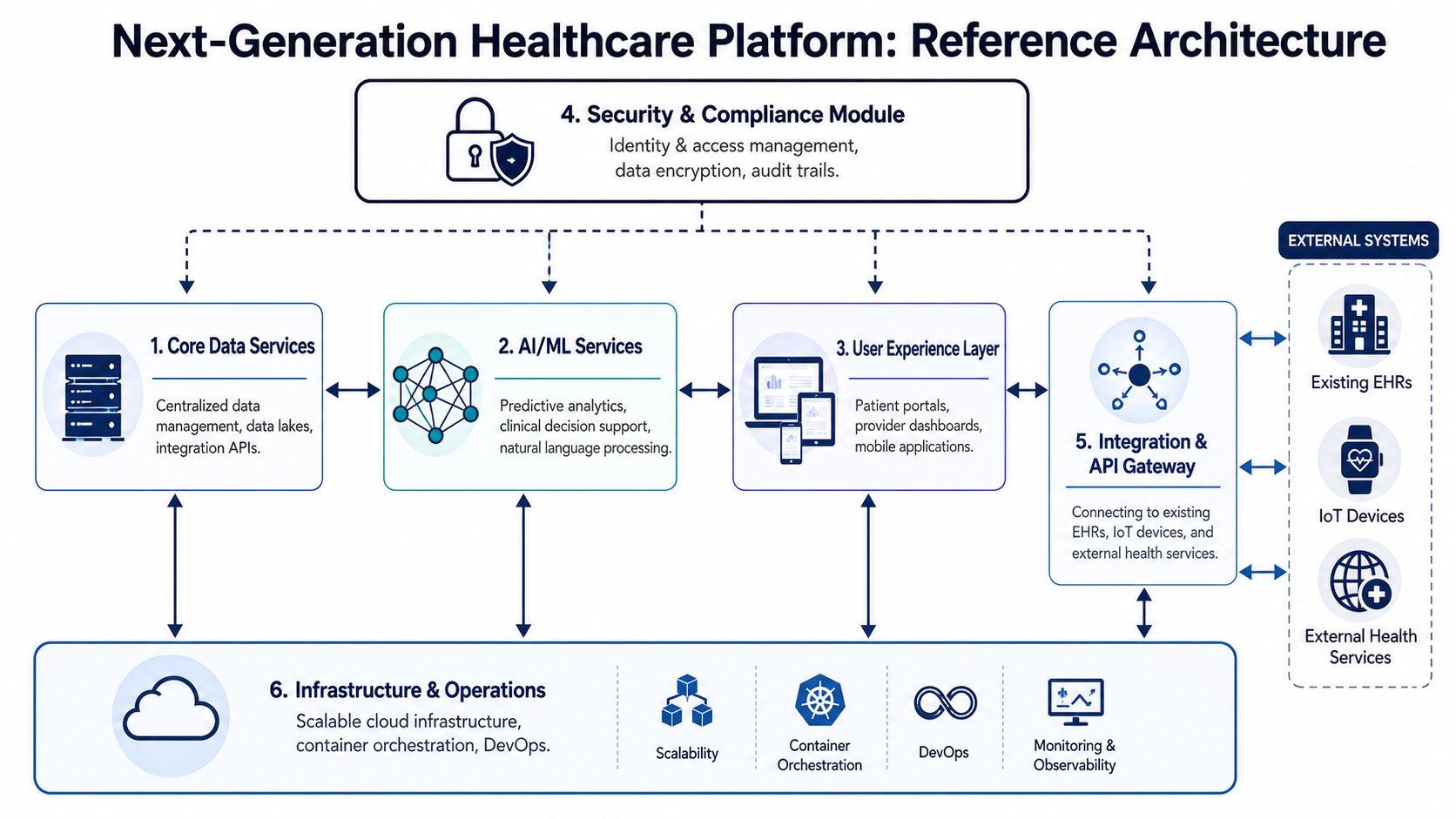
A modular stack that scales
A practical reference architecture is usually easier to manage in logical layers.
| Layer | Purpose | Typical choices |
|---|---|---|
| Data layer | Ingest, store, normalize, and govern structured and unstructured data | Cloud object storage, relational databases, warehousing tools, stream processing |
| Core services layer | Shared business capabilities such as identity, consent, scheduling, billing, messaging | Microservices on containers or managed compute |
| Intelligence layer | Analytics, rules engines, NLP, model inference, monitoring | Python services, model serving frameworks, BI tools |
| Integration layer | FHIR server, API gateway, partner connectors, event routing | API management, message brokers, interface engines |
| Presentation layer | Clinician dashboards, patient portal, admin console, mobile apps | React, Flutter, native mobile, design systems |
In cloud deployments, teams often combine Kubernetes for service orchestration, Kafka or cloud-native event buses for asynchronous processing, Python for AI services, and managed databases for reliability. What matters is less the vendor choice and more the system boundaries. Your consent service should be reusable. Your identity layer should support multiple user types. Your audit system should observe every major transaction without each team reinventing it.
Build around interfaces, not assumptions
The integration layer deserves disproportionate attention because it's where healthcare projects often stall. Legacy systems may expose HL7 feeds but not modern APIs. Partners may support FHIR selectively. Devices may send data in formats no downstream workflow can directly use.
That's why an API gateway and translation layer are foundational. They protect internal services from external inconsistency. For teams planning that layer in detail, this enterprise API integration playbook is worth reading because it frames integration as a governed product capability, not a one-off technical task.
We covered similar concerns in our guide to healthcare platform API engineering, especially around versioning, interface contracts, and keeping clinical workflows stable while integration surfaces evolve.
Technology choices that age well
A few stack decisions are usually safer than they look:
Choose managed services where they remove undifferentiated burden: Databases, logging, secrets management, and object storage rarely justify heroic reinvention.
Containerize business services: It gives you deployment consistency and clearer operational boundaries.
Keep model-serving isolated from transaction-processing paths: AI failures shouldn't block core care workflows.
Design observability early: Logs, traces, metrics, and audit events need to correlate across services.
The best healthcare architecture isn't the most advanced one. It's the one your team can secure, operate, and evolve without freezing delivery.
A Phased Roadmap for Implementation
Monday morning, the CEO wants a patient app, the clinical lead wants referral visibility, and compliance wants clearer consent controls before anything new goes live. Teams that treat all three as one giant transformation program usually end up with a late project, a brittle architecture, and tired users who stop trusting the rollout.
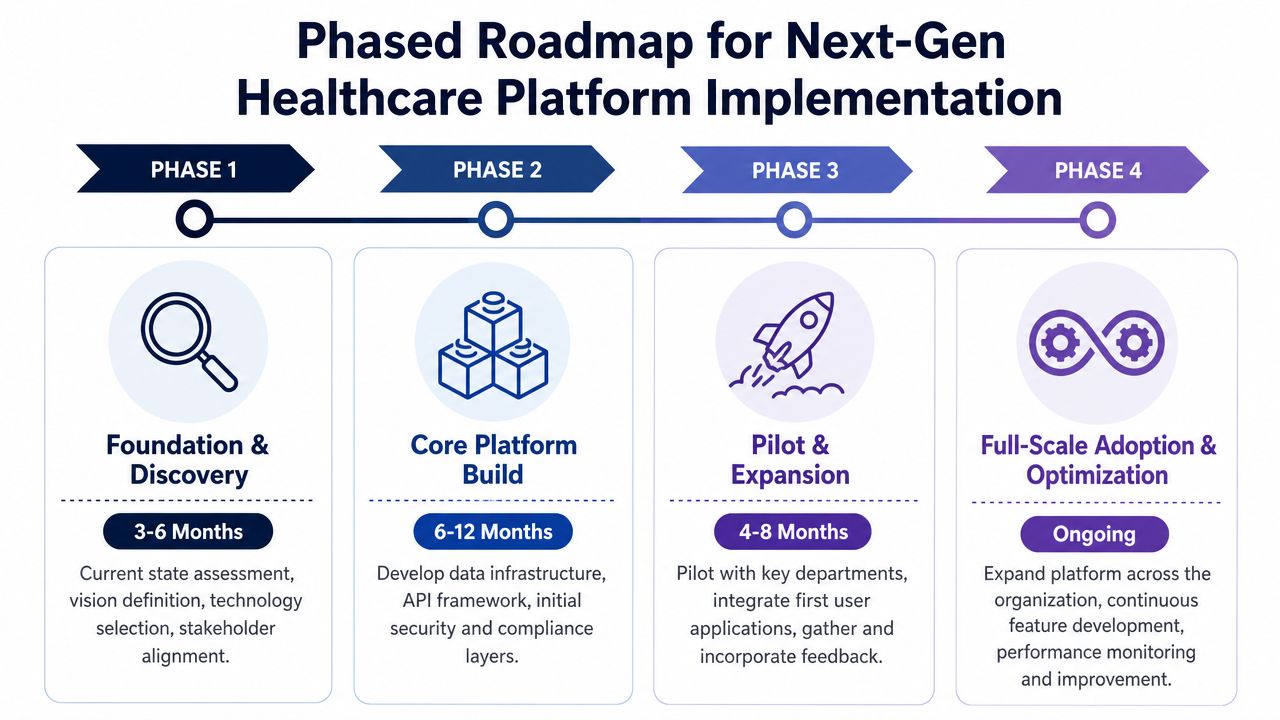
Phase 1: Foundation and discovery
Start with one care journey that already hurts. Referral coordination, chronic care follow-up, specialty intake, and discharge communication are common starting points because failure is visible, costly, and easy for staff to describe in operational terms.
This phase usually includes:
Workflow diagnosis: Map dropped handoffs, repeated data entry, approval bottlenecks, and points where staff leave the system to finish the job.
Stakeholder alignment: Get clinical, operational, legal, security, and engineering leaders to agree on what success looks like.
Architecture choices: Decide cloud posture, integration boundaries, identity approach, and what must stay decoupled from EHR dependencies.
AI scoping: Identify decisions that can tolerate probabilistic outputs and those that still require deterministic rules and human review.
I push teams to test one more assumption during discovery. Can the target users access the experience you plan to ship? A remote monitoring workflow designed around stable broadband and newer smartphones may fail in rural or under-resourced settings before any clinical value appears. Product decisions made here affect equity later.
Phase 2: Core platform build
Build the smallest production-safe foundation that can support the first workflow well. That usually means identity, role enforcement, audit trails, consent handling, core APIs, security monitoring, and a usable front end for the people doing the work.
For organizations dealing with fragmented records and aging interfaces, healthcare data modernization strategy often has to progress in parallel with platform delivery. Founders sometimes want to postpone that work. In practice, old data contracts and poor source quality show up early, usually during pilot integration and reporting.
A startup also has to make a staffing decision here. Internal team only, external build partner, or a blended model. The trade-off is straightforward. Speed without architectural discipline creates future rework. Architecture without delivery speed burns runway.
Phase 3: Pilot and expansion
The pilot should answer operational questions, not just product questions. Can staff complete the workflow with less back-and-forth? Do interface failures get detected before they disrupt care? Does consent logic hold up under real exceptions, proxy access, and edge-case user roles?
A useful pilot does three things:
Validates workflow fit: Confirm that the new process is easier than the workaround it replaces.
Exposes integration debt: Surface brittle vendor interfaces, missing events, and data fields that arrive late or malformed.
Clarifies operational ownership: Assign who resolves interface failures, user access issues, data quality defects, and patient support requests.
This is also the right time to test fairness assumptions if AI is involved. A model that performs well in one health system or patient population can break down in another. That is not just a model problem. It is a rollout problem, a governance problem, and sometimes a reimbursement problem.
Phase 4: Scale and optimize
After the first workflow proves value, expand through repeatable platform capabilities. Add departments, modules, and automation only when your shared services can support stricter uptime targets, release controls, audit requirements, and support processes.
At this stage, custom software development becomes an operating model decision rather than a build decision. Teams may also need disciplined SaaS product development if the platform must support multiple tenants, payer-provider variations, or region-specific compliance rules.
The mistake I see most often is scaling feature count faster than operational maturity. A broader rollout increases support volume, exception handling, model monitoring, and security overhead. Build for the next workflow, but verify that smaller clinics, lower-bandwidth sites, and under-resourced partners can use what you are scaling.
Start with a narrow workflow, but design shared services that can survive wider adoption, stricter oversight, and less predictable care environments.
Navigating Critical Risks and Demonstrating ROI
A lot of healthcare platform strategy still assumes that if the software is advanced enough, adoption and impact will follow. That assumption breaks down fast in underserved settings and rural environments. Technical capability doesn't create access by itself.
AI equity is a platform issue, not a policy footnote
One of the most overlooked risks is inequitable AI implementation. Under-resourced clinics often can't afford the infrastructure, training, or operational support required to adopt new tools safely. According to the California Health Care Foundation's analysis of AI equity, that gap can worsen health disparities unless organizations prioritize data diversity and reinvest part of AI project profits into IT infrastructure and training for under-resourced facilities.
That recommendation has architectural implications. If your platform strategy assumes clean, abundant, representative data from every care setting, you're already making a risky assumption. Teams need datasets that reflect differences in race, ethnicity, language, and geography, and they need governance that treats lived experience as part of model quality, not a side conversation.
Infrastructure gaps can nullify digital strategy
A telehealth feature looks impressive in a product demo. It does nothing for a clinic that can't support reliable connectivity. Research summarized in ScienceDirect reports that 60% of healthcare facilities in rural or underserved areas lack the technological infrastructure and high-speed internet needed for effective telemedicine adoption.
That should change how executives evaluate readiness. If you ignore bandwidth, device quality, and local support capacity, you may launch a platform that works beautifully in urban pilot settings and fails where access matters most.
A grounded risk review should include:
Connectivity reality: Can target facilities realistically support the intended workflow?
Operational capacity: Who handles onboarding, support, and issue resolution locally?
Accessibility burden: Are elderly patients, people with disabilities, and lower-income users being asked to carry too much technical complexity?
Fallback pathways: What happens when video fails, device sync breaks, or consent can't be captured remotely?
ROI needs a wider lens
Short-term efficiency still matters. Reduced documentation burden, fewer manual handoffs, and cleaner data pipelines all have value. But healthcare leaders make weak ROI decisions when they count only near-term labor savings and ignore access, quality, equity risk, and resilience.
A stronger ROI model includes three layers:
| ROI lens | What to assess | Why it matters |
|---|---|---|
| Operational | Workflow time, rework reduction, administrative simplification | Shows whether the platform removes friction |
| Clinical and access | Care continuity, reach across settings, patient follow-through | Captures whether the platform improves service delivery |
| Strategic risk | Compliance posture, AI bias mitigation, infrastructure sustainability | Protects long-term viability |
For compliance-heavy teams, a practical reference like this guide to automating HIPAA compliance can help frame which controls are worth systematizing instead of managing manually. The point isn't automation for its own sake. It's reducing preventable operational risk while the platform grows.
The Future of Connected and Proactive Healthcare
The future belongs to platforms that make care feel continuous instead of episodic. That means systems that can coordinate across visits, channels, devices, and organizations without making patients or clinicians reconstruct the story each time.
Younger users are already forcing that shift. In a 2024 McKinsey survey on Gen Z healthcare behavior, 77% of Gen Z respondents had considered switching providers in the previous 24 months, 42% turned to doctors for health information, and 38% relied on social media. That's not just a marketing insight. It's a platform design signal. The next front door to healthcare is digital, comparative, and shaped by consumer expectations.
The organizations that move first won't win because they deployed the flashiest AI model. They'll win because they built reliable data foundations, usable workflows, trustworthy governance, and access models that don't leave underserved settings behind.
If you want to see what transformation looks like in practice, review relevant client cases and evaluate whether your current architecture can support the care model you expect to deliver in the next few years.
Frequently Asked Questions
How can a small startup handle massive data storage and compliance requirements?
Don't build your own data center. Use a major cloud provider with compliant service options and lean on managed components for storage, databases, encryption, secrets handling, and audit support. That lets the team focus on application logic, product workflows, and validation instead of basic infrastructure maintenance.
The key is discipline. Define data classes early, isolate protected health information carefully, and make logging, access control, and retention policies part of the platform foundation.
What is the biggest challenge when integrating with a hospital's legacy systems?
Usually it's inconsistency. Many hospital environments still rely on a mix of old interfaces, partial standards support, and local workflow customizations that don't show up in procurement documents. The mistake is trying to solve every integration path at once.
Start with one high-value interface. Admission, discharge, and transfer data is often a sensible place to begin. A working first integration builds trust and reveals how the hospital really manages exceptions, mappings, and ownership.
Who owns the patient data on these platforms, and how is privacy ensured?
The patient is the core rights holder. Providers act as stewards, and the platform acts as the technology custodian. In practice, privacy depends on governance and architecture working together.
That means granular consent management, encryption in transit and at rest, strict role-based access controls, reliable audit trails, and clear policies for data sharing, retention, and deletion. Privacy fails when teams treat it as a legal document instead of an operating model.
Building a modern healthcare platform takes more than strong engineering. It takes architectural judgment, compliance discipline, and a realistic plan for interoperability, AI, and scale. If you're looking for a Bridge Global team with experience in healthcare software, platform engineering, AI-enabled product delivery, and long-horizon modernization, explore their work across custom healthcare software development, custom software development, and AI development services.
About Upendra Jith
Upendrajith completed his Master's in English and has been a commercial content developer for the past three years. He's more inclined to develop content with a 'street-smart' delivery on topics such as technology, media, or anything he can get his hands on. He has a fixation on lyrics, dark poetry, media, technology, and flow arts.
View all posts by Upendra Jith →