


Mastering Healthcare Edge Computing
By the time a health system decides it has an edge problem, it usually already has an operations problem. Device data is piling up, cloud latency is showing up in clinical workflows, and teams are being asked to keep PHI protected across endpoints that were never designed to carry that responsibility at scale.
Healthcare edge computing matters because it changes where decisions are made and where protected data is handled. For CTOs building remote monitoring platforms, imaging pipelines, Tele-ICU services, or connected medical products, that has direct consequences for uptime, breach exposure, and HIPAA scope. The architectural question is no longer whether local processing is useful. The question is which workloads should stay close to the device, which events must continue during network loss, and which controls have to be enforced before data ever reaches the cloud.
I have seen edge projects fail when teams treat them as a latency upgrade instead of a security and operating model. The stronger approach is to design edge around three constraints from the start: local resilience, minimum necessary data movement, and centralized policy control. That is what turns a pilot into an enterprise pattern instead of another isolated deployment.
For provider organizations already working through broader digital transformation in healthcare delivery and operations, edge should be evaluated as infrastructure with compliance implications, not as a feature add-on. Done well, it reduces round trips, limits unnecessary PHI transfer, and keeps critical services running during outages. Done poorly, it creates a larger endpoint estate, inconsistent patching, and new audit gaps.
The Inevitable Rise of Edge Computing in Modern Healthcare
Healthcare edge computing is best understood as a response to two operational failures in modern health IT. First, too much data is being created too far from where decisions need to happen. Second, cloud round trips often arrive too late for time-sensitive care.
That's why the market is moving so quickly. The global healthcare edge market's rise from USD 8.21 billion in 2025 to approximately USD 47.23 billion by 2035, at a projected 19.12% CAGR, signals that providers and product teams are treating edge as infrastructure, not experimentation, according to Precedence Research.
In practice, edge means processing data close to where it's produced. That might be inside a bedside monitor, on a gateway inside a hospital unit, in a local server rack, or in a compact compute appliance inside a clinic. The point isn't novelty. The point is to shorten the path between signal and action.
What edge changes operationally
A cloud-only architecture centralizes intelligence. That works well for reporting, training models, and non-urgent workflow coordination. It breaks down when software has to support immediate triage, device control, or continuous monitoring.
Edge changes the decision boundary:
-
Clinical events are evaluated locally so systems don't wait on distant infrastructure.
-
Sensitive data can stay near the source instead of crossing more networks than necessary.
-
Applications remain useful during connectivity issues rather than failing hard when cloud access degrades.
Edge isn't just a performance upgrade. It's a redesign of where responsibility lives in the system.
For teams already modernizing provider infrastructure, the pattern aligns with the broader shift described in Bridge Global's guide to digital transformation in healthcare providers. The organizations getting this right aren't buying a product and calling it done. They're redesigning workflows, governance, and deployment models around local decision-making.
The technical payoff is real. The strategic payoff is bigger. A capable healthtech software development partner helps turn edge from an isolated pilot into an operating model.
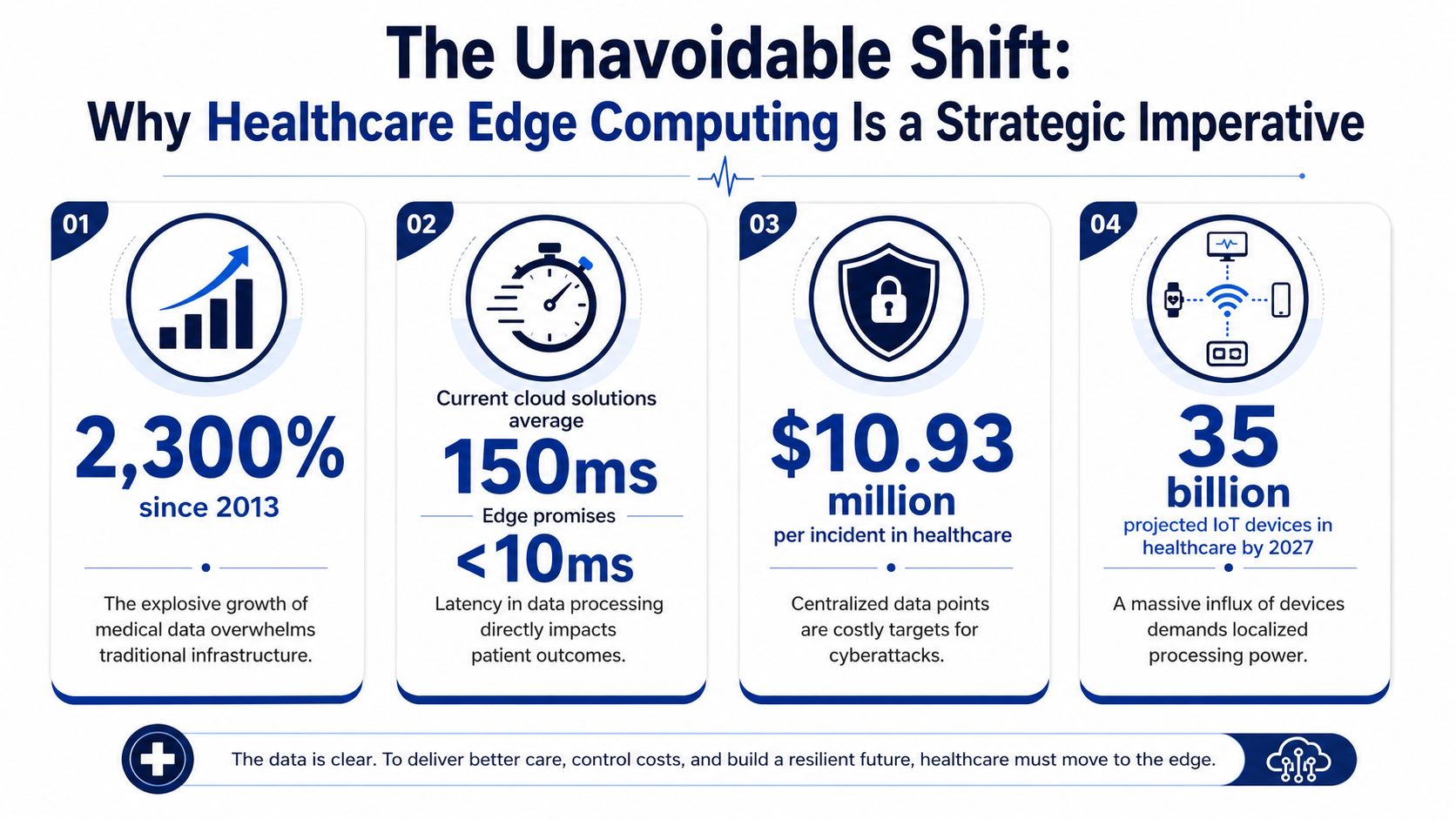
Why Edge Is Now a Strategic Imperative, Not a Technical Option
By 2025, an estimated 75% of all medical data is projected to be generated at the edge, and healthcare data volume is expected to grow at a 36% CAGR, according to NVIDIA's analysis of healthcare at the edge. NVIDIA also notes that healthcare produces roughly 30% of the world's total data volume, with about 10 billion connected medical devices in use.
For a CTO, those numbers change the architecture discussion. Edge is no longer a performance feature that can wait for a later phase. It becomes a control point for latency, security boundaries, resilience, and operating cost.
Why cloud-first design hits a limit
Cloud still belongs in the stack. It is the right place for model training, enterprise reporting, longitudinal analysis, and cross-site coordination. The problem starts when teams force time-sensitive clinical workflows through the same path as archival or analytical workloads.
A centralized design struggles once bedside devices, imaging systems, wearables, and home-monitoring kits all push continuous data upstream. In practice, the bottleneck is often not compute. It is network reliability, WAN latency, packet loss, and the operational overhead of moving protected health information across more systems than necessary.
Intel makes the operational case clearly in its overview of edge computing in healthcare. It points to emergency care and remote patient monitoring as environments where split-second response matters. That matters for clinicians, but it also matters for compliance teams. Every extra hop, queue, and integration point expands the attack surface and complicates HIPAA controls.
The strategic case is operational, financial, and regulatory
The strongest edge business cases usually show up in three places at once.
| Decision area | Cloud-only weakness | Edge advantage |
|---|---|---|
| Time-sensitive clinical response | Alerts and decisions depend on round trips to central systems | Triage, inference, and alerts run locally |
| Security and HIPAA scope | More raw PHI traverses networks and third-party services | Data can be filtered, minimized, and retained locally first |
| Resilience and uptime | Internet or WAN disruption can stall critical workflows | Local services keep running during connectivity loss |
That second row gets underestimated.
A mature edge design is not just about speed. It is often the cleanest way to apply data minimization, segment medical devices from enterprise IT, enforce local access controls, and keep sensitive workloads available even during a cloud outage. Teams that pair edge processing with a well-structured healthcare data pipeline architecture usually scale more cleanly because they decide early which data stays local, which data is summarized, and which data must move to the cloud for broader use.
Practical rule: If a workflow affects care delivery or patient safety within seconds, or if it becomes unsafe when connectivity degrades, design it to function locally first.
Where CTOs should draw the line
Not every workload belongs at the edge. Claims systems, population analytics, research datasets, and centralized AI training generally fit better in cloud or core data center environments. The mistake is treating edge as an all-or-nothing decision.
A better approach is to classify workloads by consequence of delay, tolerance for disconnection, and PHI exposure. If delayed processing causes alarm fatigue, missed intervention windows, or manual workarounds on the floor, edge deserves priority. If the workload mainly supports retrospective analysis, centralize it.
I usually advise teams to start with one question: which decisions must still happen safely if the network is slow or unavailable? That framing produces better architecture than starting with hardware procurement. It also creates a clearer path to pilot success, because the first deployment is tied to a clinical or operational outcome rather than a generic modernization goal.
Understanding Core Architectures and Key Components
Edge architecture in healthcare succeeds or fails on one decision: where clinical logic runs when networks slow down, devices misbehave, or central systems are unavailable. CTOs do not need a complicated reference model first. They need a deployment model that assigns processing, storage, security controls, and failure handling to the right tier.
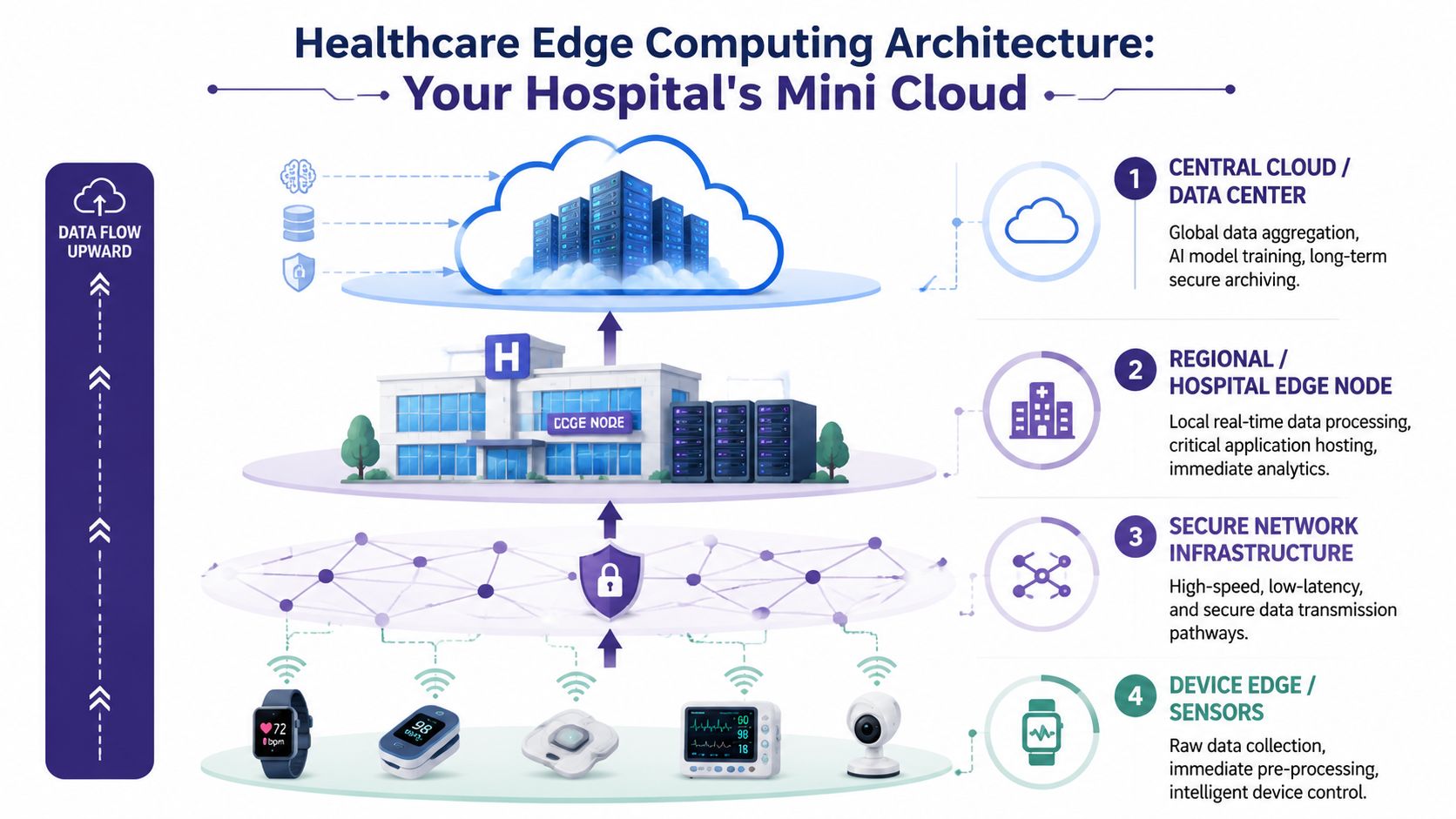
The four layers that matter
Most production deployments settle into four layers, even if vendors label them differently.
-
Device edge
Data originates here, and some first-pass processing may already happen. Bedside monitors, imaging systems, wearables, infusion pumps, and home kits can validate signals, buffer data briefly, and trigger limited local actions. -
Edge gateway
Gateways sit between devices and local applications. They aggregate traffic, normalize formats, enforce device identity, translate protocols, and reject malformed or unauthorized data before it reaches clinical workflows. -
Hospital or clinic edge node
This tier hosts the local services that cannot wait on the WAN. Common examples include inference services, alarm logic, image prioritization, short-term data stores, local APIs, and workflow services that must continue during outages. -
Central cloud or data center
Central platforms handle fleet management, enterprise reporting, long-term retention, model training, cross-site analytics, and systemwide policy distribution.
What each layer should own
The cleanest architectures keep responsibilities narrow.
-
Devices should capture and send trusted signals: Add autonomous logic only when patient safety or device certification requires it.
-
Gateways should validate, translate, and enforce policy: Avoid turning them into opaque appliances full of one-off workflow rules.
-
Edge nodes should run time-sensitive decisions: They are the right place for local inference, caching, and failover operations.
-
Cloud platforms should coordinate across sites: Use them for centralized visibility, governance, and compute-heavy tasks that do not need immediate execution.
Teams run into trouble when the same rule exists on a device, gateway, edge server, and cloud service. That creates version drift, uneven patching, and audit headaches. In a HIPAA environment, it also makes it harder to prove where PHI was processed, stored, or exposed.
The architecture choice is really a control choice
I usually frame edge design as a control question, not a hardware question. Which tier enforces identity? Which tier holds cached PHI? Which tier continues operating during downtime? Which tier receives signed updates, and how are failed rollouts reversed?
Those answers matter more than the vendor diagram.
A practical pattern looks like this:
| Architecture choice | Where it fits | Trade-off to plan for |
|---|---|---|
| Thick edge node | ICU monitoring, imaging triage, local alerting, branch sites with unstable connectivity | Strong local capability increases patching, observability, and configuration management work at each site |
| Thin edge gateway | Facilities with reliable networks and strong central operations | Lower local complexity, but weak tolerance for WAN disruption and slower local recovery |
| Hybrid split | Multi-site health systems balancing local resilience with centralized governance | Works well if data sync rules, model versioning, and downtime procedures are explicit |
Security components belong in the core design
Healthcare edge systems need the same discipline applied to cloud workloads, but with tighter physical and operational constraints. Every tier should have a defined trust boundary, encrypted communications, certificate-based identity, role-based access, centralized logging, and a documented PHI retention policy.
At the edge node, I want to see secure boot, encrypted local storage, remote attestation where feasible, and signed update packages. On gateways, I want protocol control, device allow lists, and strong segmentation from the rest of the clinical network. On the central side, I want policy orchestration, key management, audit trails, and a way to revoke compromised nodes quickly.
That design work is easier when edge is part of a broader healthcare data pipeline architecture, instead of a stand-alone infrastructure purchase.
Components CTOs should standardize early
Three components deserve early standardization because they determine whether a pilot can scale.
-
A device and workload identity model. Every node, gateway, and service needs a verifiable identity.
-
A remote operations plane. Teams need patching, configuration management, health monitoring, and rollback without sending staff onsite for routine changes.
-
A local data handling policy. Define what is processed locally, what is cached, how long it remains, and what must be forwarded, summarized, or deleted.
This matters outside classic monitoring and imaging use cases. Organizations trying to transform healthcare documentation workflows run into the same architectural questions when voice data, transcripts, and inferred clinical actions must be processed close to care delivery while still fitting enterprise security and compliance controls.
The best edge architecture is the one operations teams can patch, security teams can audit, and clinical teams can trust during degraded conditions.
High-Impact Use Cases Transforming Patient Care
The easiest way to judge healthcare edge computing is to look at where it changes care delivery, not where it looks technically elegant.
Some use cases are obvious. Others become compelling only when you follow the workflow all the way to the clinician, patient, or technician who has to act on the result.

Remote patient monitoring that can actually respond
Remote patient monitoring is one of the strongest edge fits because the value depends on timely interpretation, not just data collection. A cloud-only system can gather vitals. An edge-enabled system can assess incoming streams locally, trigger alerts quickly, and keep functioning if home connectivity becomes inconsistent.
That matters in home-based care, chronic disease management, and post-acute follow-up. It also pairs well with adjacent workflow tools. For example, teams modernizing virtual care operations often look at ways to transform healthcare documentation workflows so clinicians aren't drowning in notes while trying to respond to live patient signals.
Imaging workflows that prioritize the urgent case
Imaging is another natural edge candidate. Inference close to the scanner or within the facility can flag suspicious studies for rapid review, reduce dependency on constant upstream transmission, and shorten the distance between image capture and radiologist prioritization.
This doesn't replace central PACS, enterprise viewers, or cloud-based model training. It improves the first operational step. The system can identify which studies deserve immediate human attention before the full enterprise workflow catches up.
Tele-ICU and procedure support with less lag
Tele-ICU platforms, procedural guidance systems, and specialist-support tools all suffer when interaction feels delayed. Even when video quality is acceptable, control loops degrade if the analytics layer depends entirely on remote compute.
Edge changes that dynamic by moving portions of monitoring, event detection, and decision support inside the local environment. A specialist still collaborates remotely, but the local system does more of the immediate processing.
The right question for these workflows isn't whether cloud can support them. It's whether cloud-only support is dependable enough during the worst operational moment.
Portable imaging in underserved regions
The most important use case may be the least discussed. Edge-enabled portable AI imaging works reliably in low-bandwidth settings, eliminating repeated hospital trips and shifting radiology from hospital-centered to community-based care in underserved regions, as described by Binaytara's analysis of cancer detection in underserved communities.
That matters because it moves edge from an efficiency story to an access story. In low-resource environments, the value isn't just speed. It's the ability to deliver diagnostic capability where reliable connectivity and full imaging infrastructure aren't available.
Device intelligence without constant connectivity
Smart devices also benefit when analytics move onto or near the device. The pattern works especially well when a product has to keep operating during intermittent connectivity or when transmitting every signal upstream would be wasteful.
A few practical examples include:
-
Bedside monitoring systems that evaluate patterns locally before escalating.
-
Home-care devices that continue safe operation even if the WAN link drops.
-
Portable diagnostics that support field use in clinics with limited infrastructure.
-
Connected imaging tools that preprocess and prioritize before enterprise sync.
Teams building products in this space often combine edge capability with SaaS product development patterns for fleet management, updates, and customer-facing administration. The best implementations treat the edge device, local node, and central product platform as one product system. For broader implementation examples, it's also worth reviewing relevant client cases.
Navigating HIPAA Compliance and Security at the Edge
Security discussions around edge often collapse into slogans. “Edge is more secure” isn't good enough for a CTO, an auditor, or a compliance lead. What matters is which risks go down, which new ones appear, and how the architecture proves control.
One clear advantage is transit reduction. Localizing data processing through edge networks enhances HIPAA compliance by reducing the risk of interception during transit, because patient files, including large medical images, are stored and processed on local edge networks instead of traversing public networks, as Akamai explains in its analysis of how edge computing is transforming healthcare security.
What edge improves from a HIPAA standpoint
HIPAA work gets easier when fewer systems touch protected health information and when sensitive data travels less.
That doesn't mean edge removes compliance obligations. It means it can simplify some of the hardest ones:
-
Less data in transit reduces exposure across external pathways.
-
Local processing boundaries make it easier to define where PHI lives.
-
Selective synchronization limits how much sensitive payload reaches centralized systems.
-
On-premises or near-source handling can align better with internal residency and retention policies.
The controls that matter in practice
A secure edge deployment depends more on discipline than on product labels. The baseline should include:
| Control area | What to implement |
|---|---|
| Identity | Strong device and service identity for each node, gateway, and application |
| Encryption | End-to-end encryption in transit and encrypted storage at rest |
| Access control | Role-based access, service scoping, and least-privilege permissions |
| Auditability | Immutable logs, event histories, and traceable administrative actions |
| Update safety | Signed packages, staged rollout, and rollback capability |
Teams also need to plan for physical exposure. Edge devices may sit in clinics, hospital wings, ambulances, or patient homes. That changes the threat model. Security has to assume partial trust in the environment, not just trust in the network perimeter.
Security judgment: Edge reduces some network risks, but it expands operational responsibility. If your team can't manage device identity, patching, and audit logs well, edge will expose that weakness quickly.
How to build an audit-ready edge pattern
For HIPAA-sensitive systems, a workable approach is usually a local-first design with controlled sync to central services. Let the edge layer process clinical events and keep only the necessary data flowing outward. Use the cloud for reporting, fleet oversight, and approved secondary processing.
A few implementation habits separate solid deployments from risky ones:
-
Keep PHI local by default. Centralize only what the enterprise needs.
-
Separate inference from administration. Clinical runtime and management planes shouldn't share loose access controls.
-
Design for evidence. Every update, user action, sync event, and policy change should be traceable.
-
Plan failure behavior. Systems must degrade safely if cloud sync, identity validation, or upstream services are unavailable.
If your team is working through the broader compliance implications, Bridge Global's article on HIPAA-compliant software development is a useful technical reference.
The practical takeaway is simple. Edge can strengthen compliance posture when local processing, encryption, logging, and controlled synchronization are designed together. It becomes risky when teams move compute outward without moving governance outward with it.
Your Implementation Roadmap from Pilot to Enterprise Scale
The worst way to adopt edge is to buy hardware first and search for a use case later. The safer path is to start with one workflow where latency, resilience, or local processing changes the outcome in a visible way.
Healthcare edge computing architectures have shown a reduction in data transfer latency of 87.3%, with response times dropping from 143.7 milliseconds to 18.2 milliseconds, according to the WJARR study on healthcare edge architectures. That kind of improvement is meaningful only if you target a workflow that benefits from it.
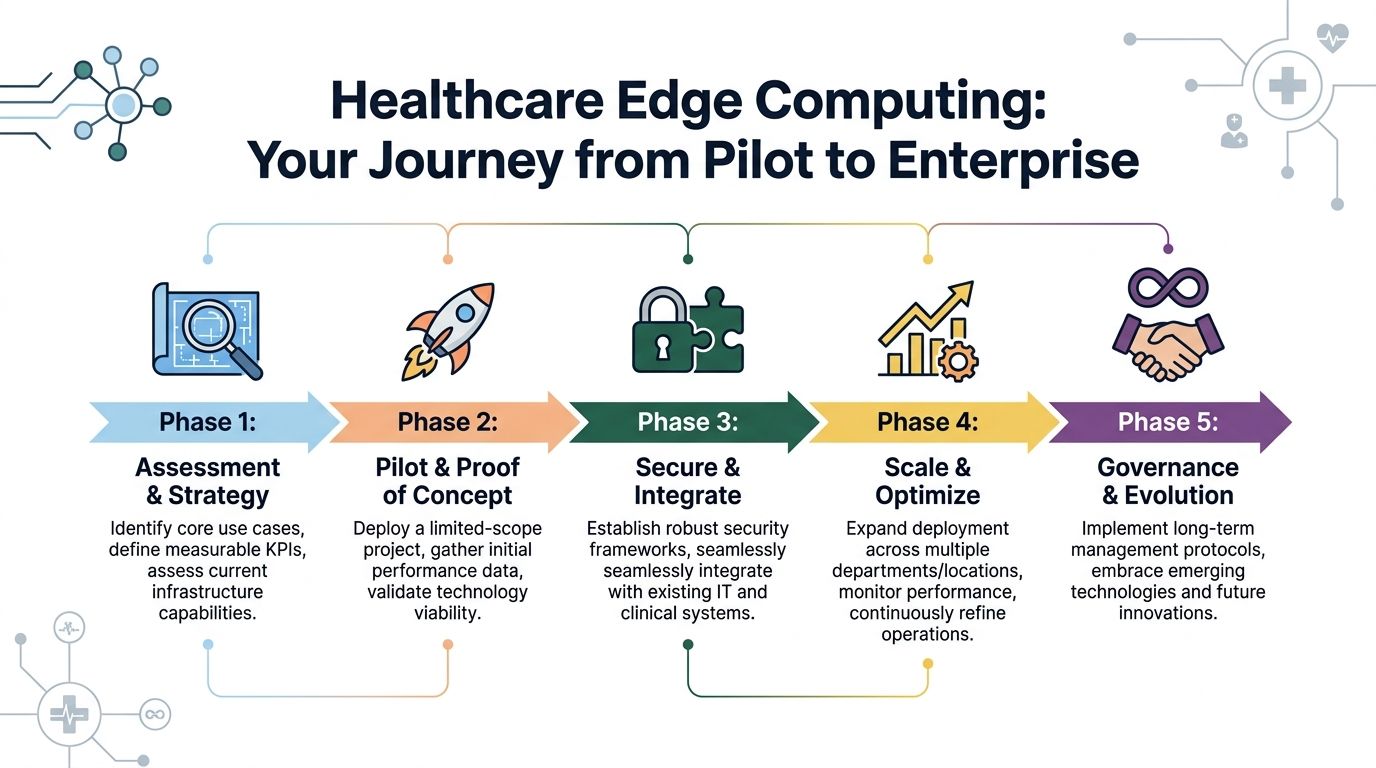
Phase one and two
Start narrow. Pick a workflow that has all three of these properties:
-
Time sensitivity such as monitoring, alerting, or image prioritization
-
Operational pain that clinicians or operators already feel
-
Clear boundaries so the pilot can be isolated without redesigning the whole enterprise
Then build a pilot with limited scope. One unit, one clinic, one device class, or one imaging stream is enough. The pilot should answer practical questions, not just technical ones. Can the local node be deployed cleanly? Can your team monitor it remotely? Can the workflow continue during connectivity disruption? Do clinicians trust the alerts?
Technology selection without overengineering
Once the pilot proves clinical and operational value, choose the stack based on supportability.
That usually means evaluating:
-
Hardware profile based on local inference, storage, and environmental constraints
-
Runtime model for containers, services, or embedded logic
-
Integration approach with EHRs, PACS, identity systems, and operational tools
-
Delivery model that fits your team's capacity and governance expectations
Different organizations will reach different conclusions here, which is why software development service models matter. A startup building a new edge-enabled product won't structure delivery the same way a provider network modernizing internal infrastructure would.
Scaling without creating a fleet nightmare
Enterprise rollout is where many promising pilots break. A useful pilot can still fail as a platform if every site needs manual tuning, custom support, or one-off policies.
Use this checkpoint list before broad rollout:
-
Standardize deployment artifacts so every node starts from the same known baseline.
-
Separate site-specific configuration from application logic to reduce drift.
-
Automate updates and rollback paths before the fleet grows.
-
Define governance for security ownership, clinical validation, and change approval.
-
Measure live performance continuously instead of treating rollout as a one-time project.
Don't scale a pilot because it worked once. Scale it because you can operate it repeatedly.
Many teams find it helpful to align edge adoption with a broader AI implementation roadmap, especially when the local node is running inference, prioritization, or assistive decision support. The implementation challenge isn't just deployment. It's repeatable operation across a distributed environment.
Integrating Edge with Your Cloud and AI Strategy
Edge isn't a replacement for cloud. It's a way to use cloud more intelligently.
The strongest healthcare platforms split responsibilities cleanly. The cloud handles the tasks that benefit from scale, central visibility, and heavier compute. The edge handles the tasks that lose value if they wait.
Deploying edge infrastructure can decrease the volume of data transmitted between endpoints and central cloud infrastructure by up to 40 to 60%, significantly lowering bandwidth costs and network congestion, according to the PMC analysis of edge deployment in IoT environments.
The hybrid model that works
A practical division of labor looks like this:
| Cloud responsibility | Edge responsibility |
|---|---|
| Long-term storage and archival | Local event processing |
| Model training and retraining | Real-time inference |
| Cross-site analytics | Immediate alerting and prioritization |
| Fleet-wide visibility | Site-level resilience |
| Enterprise reporting | Workflow continuity during network instability |
That hybrid pattern is especially useful for AI systems. Train centrally. Validate centrally. Deploy locally for fast inference. Then sync outcomes, telemetry, and selected records back to central systems for governance and improvement.
Integration points that need real attention
Most failures happen in the spaces between systems. Not inside them.
Focus on these integration questions early:
-
How will model updates reach edge nodes safely?
-
What gets synchronized immediately, and what can wait?
-
How will local identifiers map to enterprise records?
-
What happens when an edge node falls behind on updates?
-
Which system is authoritative during temporary conflicts?
Mature enterprise AI solutions, experienced AI development services, and reliable healthcare integrations are central to execution. The hard part isn’t proving that local inference works. It’s making sure updates, records, and governance stay coherent across the distributed estate.
For teams working through broader platform operations, this external guide on solving cloud infrastructure challenges is a practical companion because many edge problems are really cloud management problems expressed at the network boundary.
A design principle worth keeping
Keep the cloud authoritative for governance. Keep the edge authoritative for immediacy.
That separation avoids two common mistakes. One is pushing every decision upward and creating latency. The other is pushing too much autonomy outward and losing consistency across sites. Good architecture chooses the decision location based on urgency, not ideology.
Frequently Asked Questions About Healthcare Edge Computing
Is healthcare edge computing only for large hospital networks?
No. Smaller providers, startups, and medical device companies often have some of the clearest edge use cases because they’re building focused workflows. A remote monitoring product, portable diagnostic platform, or imaging triage system may benefit from edge sooner than a broad enterprise platform does.
The key is to avoid adopting edge as a trend. Adopt it when the product or workflow needs local processing, lower latency, better resilience, or tighter control over sensitive data movement.
Does edge reduce the need for cloud infrastructure?
It changes the cloud’s role more than it reduces the need for it. You’ll still need centralized services for governance, analytics, storage, model training, reporting, and enterprise integration. What changes is that the cloud no longer has to sit in the critical path of every immediate decision.
That shift often produces a healthier architecture because each layer gets a clearer job.
What’s the first use case a CTO should evaluate?
Start with a workflow that suffers when connectivity, latency, or bandwidth becomes unreliable. Good candidates often include remote patient monitoring, imaging prioritization, smart device workflows, and local decision support in high-acuity settings.
If the team can’t explain exactly which delay or dependency edge removes, the use case probably isn’t ready.
Is edge harder to secure than cloud?
It’s different to secure. Some risks go down because less sensitive data has to travel across broader networks. Other risks go up because you now have distributed assets, local runtimes, and a larger operational footprint.
In practice, security success depends on strong identity, encryption, access control, logging, patch discipline, and safe update mechanisms. Teams that already operate with those controls tend to do well at the edge. Teams that rely on informal processes struggle.
How do you avoid pilot purgatory?
Pilot purgatory happens when a team proves that the technology works but never proves that the operating model works. To avoid that, design the pilot around repeatability from day one. Standardize deployment artifacts, define ownership, plan update workflows, and make sure support teams can monitor and troubleshoot remotely.
A pilot should validate not only the use case, but also the path to fleet operation.
Should edge inference live on the device or on a nearby node?
It depends on the workflow. Device-level inference can work well when autonomy is essential, and the device has enough compute. A nearby node is often better when multiple devices feed the same workflow, when models are heavier, or when you want easier update management.
The deciding factors are usually latency tolerance, supportability, hardware constraints, and failure behavior.
How should teams handle compliance evidence across many sites?
Treat evidence generation as part of the platform, not as an afterthought. You need traceable logs, controlled updates, role-based access, and a reliable way to show what software and policies were active at each site.
If evidence depends on manual collection, the system won’t stay audit-ready for long.
When should a company bring in an external engineering partner?
Bring one in when the challenge spans architecture, compliance, integrations, and scale at the same time. Edge projects often fail because organizations split ownership across too many teams with no common operating model.
A good partner helps tighten system boundaries, reduce implementation risk, and build for repeatable rollout instead of one-off success.
Healthcare edge computing only pays off when it’s implemented with architectural discipline, compliance depth, and a realistic path to scale. If you’re evaluating a pilot, redesigning a clinical platform, or building an edge-enabled product, Bridge Global can help as a healthtech software development partner with expertise in custom healthcare software development, custom software development, AI-led engineering, and audit-ready delivery.
About Preethi Saro Philip
Preethi Saro Philip is a Post Graduate Research Degree holder in Economics with more than 10 years of experience in writing, editing, research and teaching. She has an intense passion for content crafting and calls herself a ‘wordsmith’. She enjoys writing on wide-ranging topics including business, technology, health & lifestyle, education, environment etc.
View all posts by Preethi Saro Philip →