


A Guide to Digital Transformation in Healthcare Providers
Hospitals generate extraordinary amounts of information, yet most of it still never shapes a clinical decision, an operational workflow, or a patient conversation. One healthcare analysis cites a World Economic Forum figure that hospitals now produce data equal to 2.3 trillion DVDs each year, while 97% goes unused, and notes that 65% of U.S. hospitals use AI-assisted predictive tools embedded in EHR systems, 47% of health organizations have implemented generative AI, and 38% are actively pursuing GenAI proofs of concept (TierPoint).
That is the context for digital transformation in healthcare providers. The issue isn't whether care organizations have software. It's whether they can turn fragmented systems, underused data, and inconsistent workflows into safer, faster, more measurable care delivery.
For executives, this shifts the conversation. The hard part isn't buying another platform. It's deciding what to standardize, what to integrate, what to automate, and how to prove that the change improved care rather than adding only screens and subscriptions.
What Is Digital Transformation in Healthcare
Digital transformation in healthcare isn't the same as digitization. Scanning a paper chart into an electronic archive is digitization. Using shared clinical data, patient-facing tools, analytics, and workflow automation to improve how care is delivered is a transformation.
A useful way to define it is this. Digital transformation in healthcare providers is an operating model change that uses connected technology, governed data, and redesigned workflows to improve patient experience, clinical coordination, and organizational performance.
The scale of the shift is hard to ignore. One industry analysis estimates that the global digital health market grew from about $175 billion in 2021 to more than $657.5 billion by 2025, while a Deloitte survey cited in the same source found 92% of respondents named better patient experience as the top desired outcome, with 76% prioritizing insights and analytics, 68% virtual health services, and 56% cloud capabilities (Sermo).
From records to real-time care models
The early wave centered on EHR adoption and online patient portals. That mattered because it moved providers away from paper-bound operations and toward connected digital systems.
What matters now is what happens after that foundation exists. Providers are trying to move from retrospective reporting to near real-time visibility, from isolated departmental systems to interoperable workflows, and from one-off technology projects to coordinated service delivery.
Practical rule: If a program doesn't change how clinicians, staff, or patients actually work, it isn't transformation. It's software deployment.
That's why platform choices alone rarely solve the problem. The stronger starting point is usually a clear architecture, a governance model, and a delivery partner that understands clinical reality as well as engineering. For organizations evaluating that path, selecting a healthtech software development partner often becomes the first strategic decision, not the last.
Connected care also reaches beyond the EHR. Remote monitoring, device data, and ambient capture are part of the same transition, which is why approaches like modernizing healthcare with IoT solutions are increasingly relevant when providers rethink their digital operating model.
Core Drivers and Benefits of Going Digital
Healthcare leaders rarely start a transformation because the technology looks interesting. They move because the existing model creates friction across care delivery, workforce capacity, and patient access.
Internal pressure comes first
Inside most provider organizations, the first pressure point is workflow fragmentation. Clinical teams document in one system, coordinate care in another, track operations in spreadsheets, and chase missing information across departments. That fragmentation slows decisions and weakens accountability.
The second pressure point is underused data. When information sits in disconnected systems, analytics teams spend their time reconciling records instead of generating insight. Executives then receive lagging reports, not operational signals they can act on.
A third pressure point is scale. As services expand across in-person, hybrid, and virtual models, old processes stop holding up. Manual scheduling, inconsistent triage, and disconnected messaging don't fail all at once. They fail one queue, one clinic, one handoff at a time.
External expectations are changing too
Patients increasingly expect healthcare interactions to work more like other digital services they already use. They want easier intake, faster communication, clearer next steps, and less repetition.
Executives are responding accordingly. Deloitte survey findings cited in healthcare analysis show that providers prioritize patient experience, insights and analytics, virtual health, and cloud capabilities as major digital transformation outcomes and investments. That combination matters because it ties front-end experience directly to back-end infrastructure instead of treating them as separate agendas.
For organizations building around those priorities, custom healthcare software development becomes relevant when off-the-shelf tools can't support the exact workflow, integration, or data governance model the provider needs.
Where the benefits actually show up
The benefits of going digital are usually most visible in four areas:
-
Care coordination improves: Teams can access the same patient context across settings instead of relying on delayed, manual handoffs.
-
Operational work becomes more manageable: Scheduling, intake, documentation support, and routine follow-up can be standardized and partially automated.
-
Patient engagement gets stronger: Portals, messaging, telehealth, and digital front-door capabilities reduce friction in access and communication.
-
Management decisions get sharper: Unified reporting and event-level data help leaders track performance with more confidence.
Providers usually see the most value when they redesign the workflow around the technology, not when they layer technology onto a broken workflow.
There are trade-offs. More tools can create more noise if governance is weak. Faster access to data can increase risk if permissions are sloppy. Virtual care can improve access but expose process gaps in follow-up and escalation. The upside is real, but it only appears when the provider treats digital transformation as a clinical and operational redesign effort, not an IT modernization program alone.
The Seven Pillars of Healthcare Digital Transformation
A provider's digital model works when several capabilities reinforce each other. Treated in isolation, each pillar helps. Connected properly, they become a durable transformation stack.
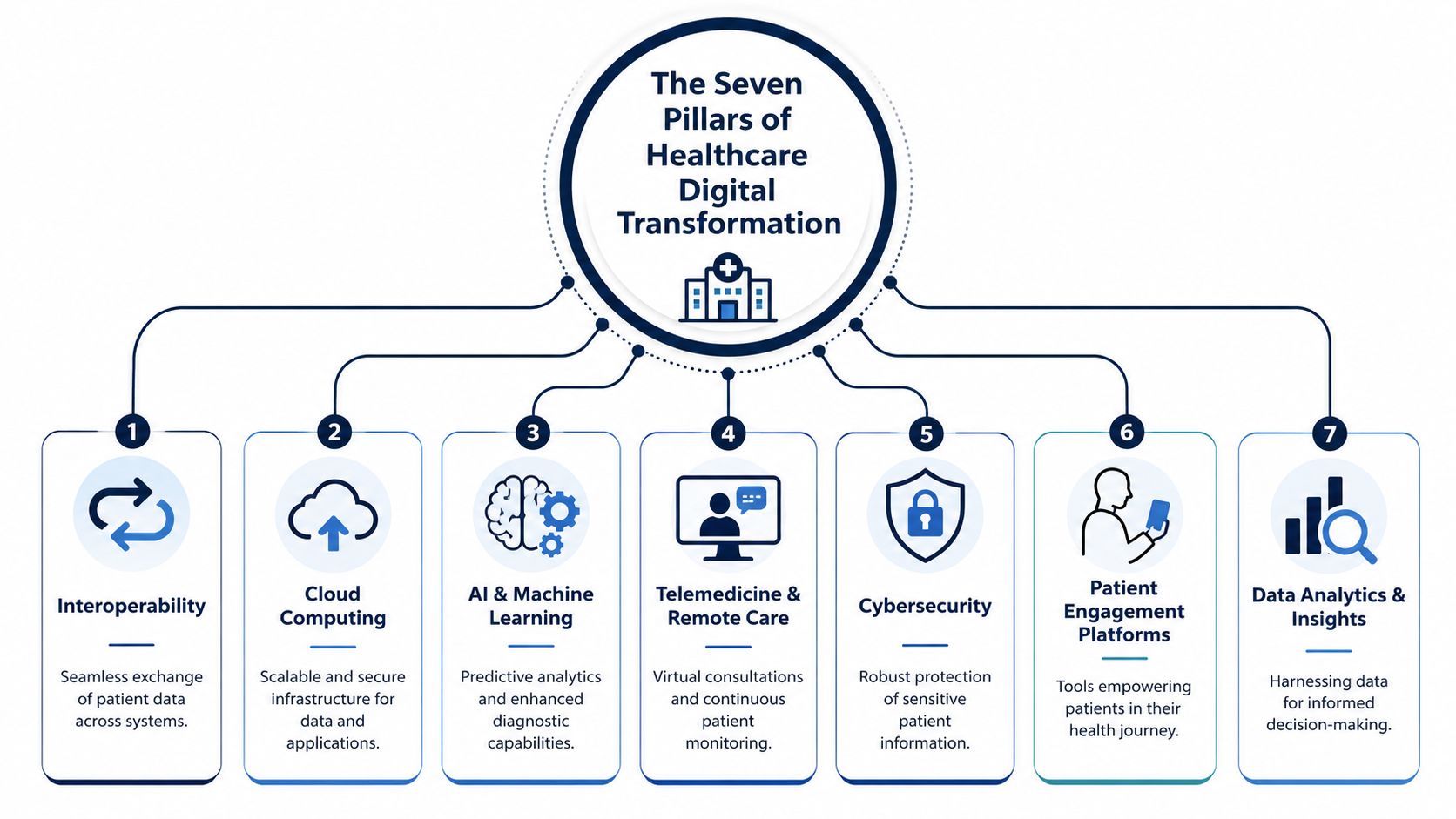
The foundational layer
EHR modernization is still the base. Many providers already have an EHR, but that doesn't mean the environment is modern. The practical question is whether the EHR supports clean data structures, usable workflows, and reliable downstream access.
Interoperability is the central nervous system. It allows clinical, administrative, and patient-facing systems to exchange data in a governed way. Without it, every other investment becomes harder to scale.
Cloud infrastructure gives providers room to standardize environments, support elastic workloads, and centralize data and application management. Cloud alone doesn't create value, but it often makes the rest of the architecture feasible.
The intelligence layer
AI and machine learning turn captured data into operational or clinical assistance. That includes predictive support inside EHR workflows, summarization, triage support, and administrative automation. The demand is obvious, but the architecture has to be ready first.
Business intelligence and analytics sit closer to management action. BI matters because executives need shared definitions, trusted metrics, and near real-time visibility into service lines, throughput, utilization, and quality.
One of the clearest signals in the market is that providers now have both a data glut and a growing appetite to use it. As noted earlier, hospitals generate huge data volumes, and one analysis reports that much of it remains unused while AI adoption inside EHR environments and GenAI implementation continue to spread. That is why the architecture question matters more than the tool question.
For teams working through sequencing, an AI implementation roadmap is useful only if it starts with data readiness, governance, workflow fit, and rollout controls rather than jumping straight to model selection.
The care delivery layer
Telemedicine and remote care extend access, but their real value appears when virtual touchpoints connect back into scheduling, documentation, escalation, and follow-up.
Patient engagement platforms include portals, intake, communication workflows, education, and self-service experiences. Done well, they reduce friction for both patients and staff.
Cybersecurity belongs in the pillar model even when teams treat it as a separate workstream. In healthcare, security isn't a back-office add-on. It's part of whether clinicians trust the system and whether patients will use it.
How the pillars work together
A mature stack usually follows this pattern:
-
Core systems hold the record of care
-
Interoperability moves the data
-
Cloud and security support scale and resilience
-
Analytics and AI create usable intelligence
-
Patient and clinician tools turn that intelligence into action
The winning architecture isn't the one with the most components. It's the one that lets the right data move to the right workflow with the right controls.
That's also where provider strategy meets build strategy. Some organizations can configure existing platforms. Others need enterprise AI solutions, customized integrations, or AI development services to operationalize a specific care or workflow model. The right answer depends less on hype and more on the constraints of the clinical environment.
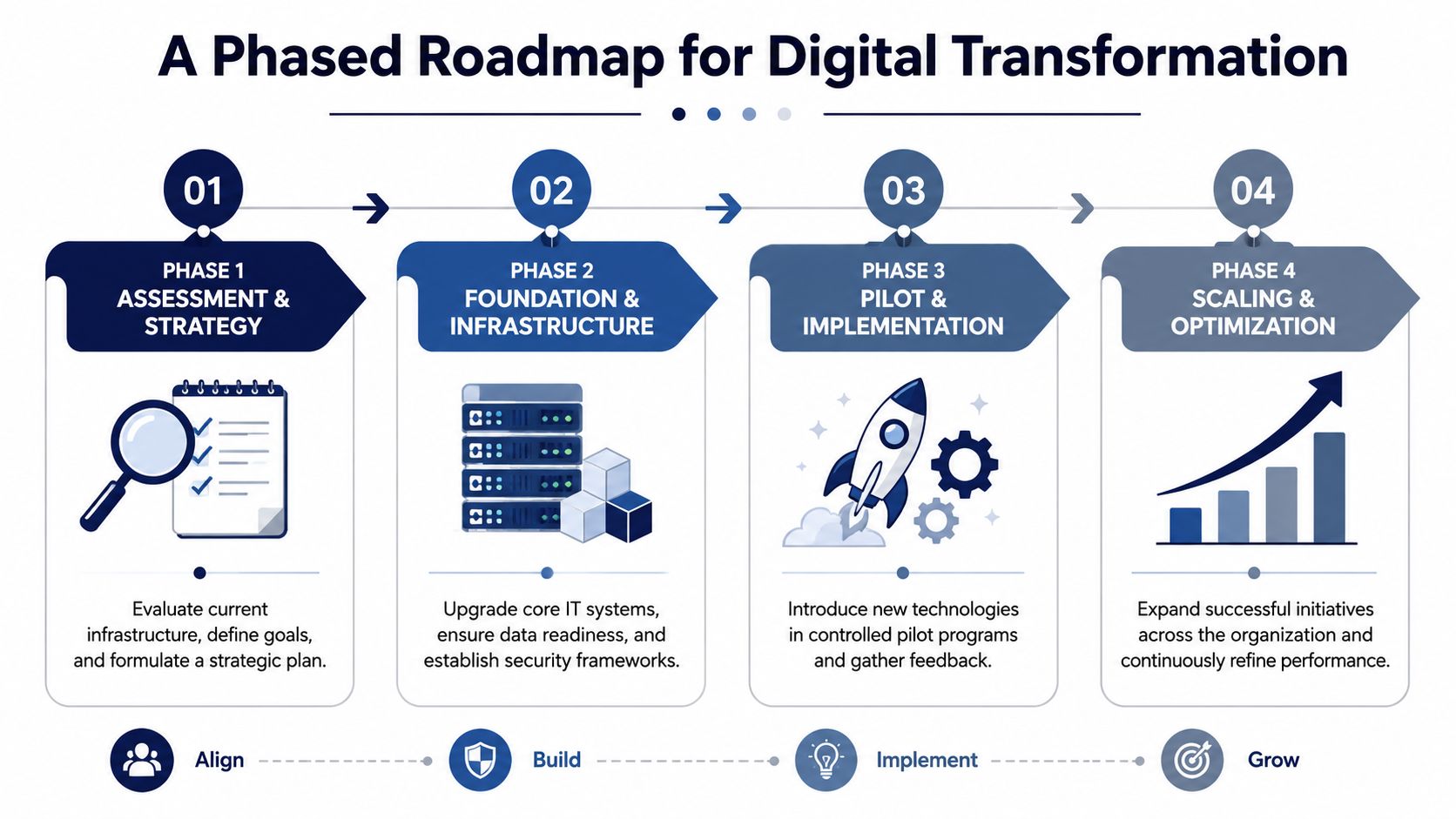
A Phased Roadmap for Implementation
Most failed transformation efforts don't fail because the vision was wrong. They fail because leaders try to change architecture, workflows, and user behavior all at once without sequencing the work.
A better approach is phased execution with clear exit criteria between stages. Deloitte reports that health systems are prioritizing insights and analytics (76%), virtual health (68%), and cloud (56%), and emphasizes the value of a governed interoperability stack that creates unified data and BI capabilities for real-time analytics and AI (Deloitte).
Phase one starts with business reality
Assessment should map three things together: current-state workflows, data flow, and business priorities. If those are assessed separately, the strategy usually breaks.
Leaders need to identify where delays, rework, duplicate documentation, and blind spots occur. They also need to define what success means in practical terms. Better experience, lower friction, faster coordination, safer transitions, or stronger reporting are all valid targets, but they need operational definitions.
A solid first phase usually includes:
-
Workflow mapping: Follow the patient journey and the staff journey, not just the system architecture.
-
Data inventory: Identify where core data originates, where it gets duplicated, and where it becomes unreliable.
-
Use-case prioritization: Rank opportunities by impact, feasibility, and adoption risk.
Phase two builds the foundation
Many organizations frequently become impatient. They want visible innovation before they've stabilized the basics.
Foundation work includes integration patterns, identity and access controls, environment planning, reporting definitions, auditability, and security architecture. It also includes deciding what should stay in the core EHR, what belongs in adjacent systems, and what needs custom development.
That's often where choices around custom software development, package configuration, or healthcare integrations become decisive. If those decisions are deferred, pilots may launch quickly but won't scale cleanly.
Phase three proves the model in a controlled setting
Pilots work when they are small enough to manage and important enough to matter. A pilot should test workflow fit, adoption behavior, data quality, and operational support, not just technical functionality.
The strongest pilots share a few traits:
-
Clear scope: One service line, one workflow, or one patient segment.
-
Named owners: Clinical, operational, technical, and compliance responsibilities should be explicit.
-
Fast feedback loops: Users need a way to report friction while the rollout is still adjustable.
Don't ask a pilot to prove everything. Ask it to prove that a defined workflow can work safely, consistently, and measurably in the real environment.
Phase four scales what the organization can govern
Scaling isn't a copy-paste exercise. It requires change management, training, operating support, and metric discipline.
At this stage, provider organizations often benefit from formal delivery structures, including product ownership, cross-functional governance, and repeatable delivery models. That's where different software development service models can help match execution capacity to the provider's internal maturity, whether the need is embedded teams, project delivery, or ongoing product support.
The key lesson is simple. Technology rollout should follow organizational readiness, not the other way around.
Navigating Governance Compliance and Security

Governance is where many digital programs become either scalable or fragile. In healthcare, every new integration, patient touchpoint, AI feature, or cloud workflow creates a trust question. Who can access what, under which conditions, and with what accountability?
The practical mistake is treating governance as a review step near the end. By then, teams are defending decisions they've already embedded into architecture and workflow design.
Governance should shape the build from day one
A durable model usually includes data classification, access control standards, audit trails, approval pathways for new data uses, vendor review, and rules for model oversight where AI is involved. Those aren't paperwork exercises. They determine whether the provider can scale services without creating operational and compliance risk.
Security design also has to cover the full surface area of the transformation effort:
-
Application layer: Role-based permissions, secure sessions, and reliable logging
-
Integration layer: Controlled interfaces, monitored data exchange, and fail-safe handling
-
Infrastructure layer: Protected cloud environments, resilient backups, and environment separation
-
Endpoint layer: Device management, remote access controls, and monitoring for unusual behavior
Compliance becomes easier when architecture is cleaner
Organizations often assume governance slows innovation. In practice, weak governance slows it down more. Every unclear approval rule, every undocumented data flow, and every ad hoc interface creates delays later.
A provider that knows where regulated data sits, how it moves, and who owns each integration can launch new capabilities faster because decision paths are already defined. That is especially true when AI is added to clinical or administrative workflows, where explainability, oversight, and security need a formal operating model.
For teams evaluating those controls in regulated environments, guidance on AI regulatory compliance and security in medtech is relevant because it addresses the overlap between technical implementation and risk management.
Secure systems earn adoption. Clinicians and patients won't trust digital tools that feel opaque, unstable, or poorly controlled.
That's why governance should be framed as an enabler. It protects patient trust, reduces execution risk, and gives executives a more stable base for long-term innovation.
Measuring Success and Avoiding Common Pitfalls
Too many provider organizations measure digital programs by launch activity: how many users logged in, how many appointments went through the portal, and how many teams completed training.
Those indicators matter, but they don't answer the hard question. Did care delivery improve?
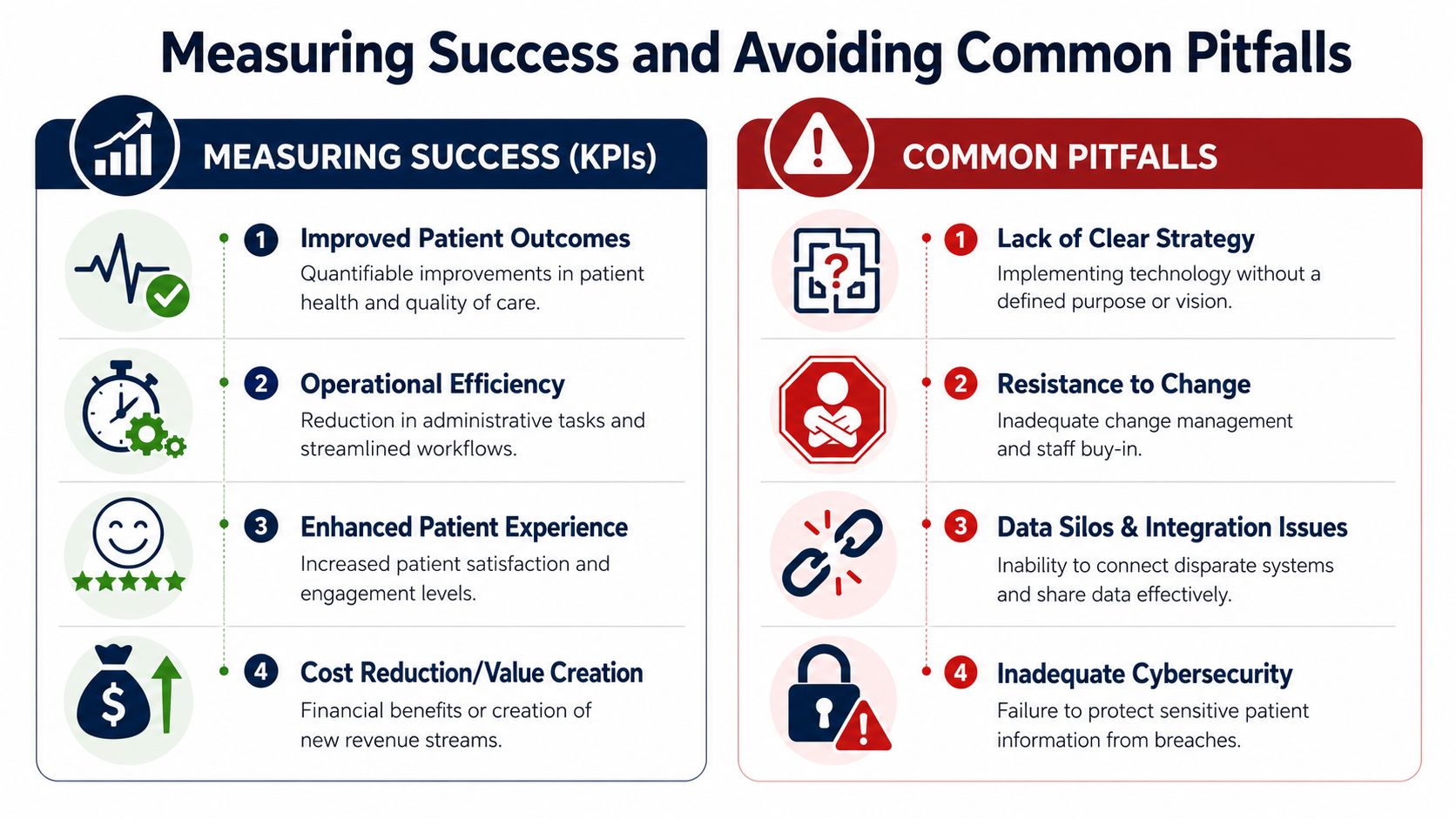
Measure across four outcome domains
A useful scorecard includes clinical, operational, patient, and financial measures. The exact metrics vary by provider and use case, but the categories shouldn't.
| Outcome area | What to examine |
|---|---|
| Clinical performance | Continuity of care, follow-up reliability, escalation timeliness, decision support usefulness |
| Operational performance | Throughput, handoff quality, scheduling friction, documentation burden, queue management |
| Patient experience | Ease of access, communication consistency, acceptance of digital channels, drop-off points |
| Business impact | Service capacity, cost-to-serve patterns, rework reduction, long-term sustainability |
One reason this matters is that healthcare leaders need stronger evidence on what digital tools are changing in practice. Recent nursing-leader research notes that telehealth, remote monitoring, AI decision support, and virtual nursing are expanding, but it also says more evidence is needed on their practical implications, including efficacy, cost-effectiveness, and patient acceptance across care models (Nature).
The most common failure patterns
The pitfalls are usually familiar, but they still derail programs:
-
Technology-first strategy: Teams select tools before they define the workflow problem.
-
Weak change management: Training happens once, feedback is shallow, and local champions are missing.
-
New data silos: A digital initiative adds another platform without solving the integration gap.
-
Poor vendor fit: A technically capable supplier may still fail if they don't understand healthcare operations.
One practical way to avoid those failures is to review how potential vendors have handled similar complexity before. Looking at client cases won't answer everything, but it helps test whether the partner has worked through regulated workflows, integration-heavy environments, and long delivery cycles.
Track whether work got easier, safer, and more reliable. If you only track usage, you'll miss whether the organization actually improved.
Success in digital transformation in healthcare providers isn't just about system adoption. It's about measurable improvement in care and operations, sustained over time.
Choosing Your Partner and Taking the First Step
Partner selection shapes the program long before the first release goes live. In healthcare, the wrong partner doesn't just create technical debt. They can create governance debt, workflow debt, and adoption debt.
What to look for in a transformation partner
The shortlist should be strict. Providers need a partner that can handle regulated environments, complex workflows, and long-term product evolution.
Look for these capabilities:
-
Healthcare domain fluency: The team should understand clinical workflows, administrative processes, and the practical aspects of patient-facing systems.
-
Integration depth: Providers rarely need a standalone app. They need connected systems, governed APIs, and clean data movement.
-
Security and compliance discipline: This has to be visible in delivery practice, not just sales language.
-
Flexible execution model: The engagement should fit the provider's internal capabilities and pace.
For some organizations, that means using a specialized vendor for a defined product or workflow. For others, it means combining internal teams with external build capacity for platform work, analytics, or AI-enabled services. Options can include SaaS product development for new provider-facing platforms or workflow systems, especially when the organization is building beyond standard package software.
Questions worth asking before you sign
A practical due diligence conversation should cover:
-
How do you handle workflow discovery with clinicians and operations leaders?
-
How do you approach integration design in healthcare environments?
-
What does your change-management support look like after launch?
-
How do you structure delivery when priorities shift mid-program?
-
How do you evidence security, auditability, and release discipline?
One option in this market is Bridge Global, which provides healthcare-focused software development, AI-enabled delivery, and product engineering across custom platforms, integrations, analytics, and compliant digital solutions. That matters if a provider needs one partner across strategy, build, and iteration rather than separate vendors for each stage.
The first step should be small and serious
The best first move usually isn't a broad platform replacement. It's a focused assessment tied to one high-friction workflow.
Start with a short list:
-
Pick one workflow with visible pain
-
Define what better looks like in operational terms
-
Map data dependencies and governance constraints
-
Choose a pilot that can be measured and supported
If your team is already considering AI, treat it as one component of the operating model, not the center of it. That's the same principle we've emphasized elsewhere in our guide to implementation planning. Strategy first, readiness second, rollout third.
Frequently Asked Questions
The hardest questions in digital transformation usually aren't technical. They're operational. Leaders need to know how to prove value, how to earn clinician trust, and how to keep innovation from creating new risk.
Below is a practical FAQ focused on those decisions.
| Question | Answer |
|---|---|
| How do we know whether digital transformation is improving care and not just digitizing workflows? | Start with outcome measures tied to a specific workflow. Look at continuity of care, clinician workload, patient acceptance, and financial impact rather than adoption alone. If a digital tool increases clicks, adds duplicate reviews, or creates more handoffs, it may be digitizing work without improving care. |
| What should we measure first after launch? | Measure a small set of indicators across operational performance, patient experience, and business impact. Keep the metric set narrow enough that leaders can act on it. Adoption can be included, but it shouldn't be the primary proof of success. |
| Why do clinician adoption problems persist even when the technology works? | Because adoption is rarely just a usability issue. Research on digital health use highlights recurring gaps around digital-health literacy, privacy and security concerns, lack of familiarity with tools, and interoperability problems. That's why the more useful question isn't which technology to buy, but how to get clinicians and patients to use it safely and consistently (Frontiers in Digital Health). |
| How do we improve trust in AI-enabled care tools? | Build trust through governance, visibility, and workflow fit. Users need to know what the tool does, when to rely on it, when to override it, and how decisions are monitored. Interdisciplinary collaboration matters here, and involving nurses in solution design helps surface practical issues that purely technical teams miss. |
| Should we start with AI or with interoperability? | Start with the constraint that most limits value. In many provider environments, interoperability comes first because disconnected data weakens every downstream use case. If data movement, identity resolution, and governance are unstable, AI features usually add noise before they add value. |
| What makes a pilot worth doing? | A good pilot tests a meaningful workflow in a real environment with named owners, controlled scope, and measurable outcomes. It should answer whether the process is safe, usable, and operationally supportable, not just whether the software runs. |
| How do we avoid creating new data silos during transformation? | Define the data model, integration pattern, and reporting ownership before expanding the toolset. Many organizations create fresh silos because each team buys or builds locally. Shared architecture review and governance are what prevent that pattern. |
| Who should own digital transformation inside a provider organization? | It should be shared across executive, clinical, operational, and technical leadership. If one function owns it alone, the program usually skews too heavily toward either compliance, IT delivery, or departmental preferences. A cross-functional governance model keeps priorities aligned. |
| How much change management is enough? | More than most teams plan for. Training should be role-specific, reinforced after launch, and linked to real workflow scenarios. Feedback loops are just as important as training content, because adoption issues often appear only after the system meets live operational pressure. |
| What's the best first use case? | Pick one with visible friction, measurable impact, and manageable integration complexity. Good starting points often sit where patient communication, staff workload, and data handoffs intersect. The right first use case is the one your organization can govern, support, and learn from quickly. |
The common thread in these questions is straightforward. Sustainable digital transformation in healthcare providers depends less on feature volume and more on disciplined execution, credible measurement, and trusted adoption.
If you’re evaluating the next step, Bridge Global can support healthcare organizations that need a practical transformation path across product strategy, compliant engineering, AI-enabled delivery, and integration-heavy platform work. The best starting point is usually a focused discovery effort around one high-friction workflow, one measurable outcome set, and one roadmap you can realistically govern and scale.
About Upendra Jith
Upendrajith completed his Master's in English and has been a commercial content developer for the past three years. He's more inclined to develop content with a 'street-smart' delivery on topics such as technology, media, or anything he can get his hands on. He has a fixation on lyrics, dark poetry, media, technology, and flow arts.
View all posts by Upendra Jith →