


Choosing Your Healthcare Technology Engineering Partner
Healthcare leaders don’t need another coding vendor. They need a partner who can help them make high-risk technology decisions under regulatory pressure, with clinical workflows, security exposure, interoperability constraints, and AI expectations all colliding at once.
The market itself explains why the old model is breaking down. The global healthcare IT market was valued at USD 420.23 billion in 2024 and is projected to reach USD 961.26 billion by 2030, growing at a 14.9% CAGR according to MarketsandMarkets’ healthcare IT market analysis. That growth is tied to cloud adoption and AI, which means architecture and compliance decisions now shape business outcomes, not just delivery schedules.
The Evolving Role of Healthtech Partners in 2026
Healthcare IT spending is rising fast, but the bigger shift is operational. By 2026, health systems, payers, and digital health companies are asking engineering partners to influence architecture, risk, compliance, and rollout decisions long before a release plan is approved.
That change is critical because modern healthcare products rarely fail on feature delivery alone. They fail at the points where privacy rules, clinical workflow, fragmented data, and integration reality collide.
A serious healthcare technology engineering partner works at that intersection. The job is not limited to shipping tickets. It includes pressure-testing assumptions, identifying where AI adds measurable value versus governance burden, and deciding which interoperability choices will hold up once the product connects to real EHR, billing, identity, and device ecosystems.
I’ve seen this shift most clearly in projects that start as straightforward application builds and turn into operating model decisions. A patient engagement app becomes a consent and identity problem. A clinician tool becomes a workflow adoption problem. An AI feature becomes a documentation, auditability, and model monitoring problem. Teams that see only the backlog usually catch those issues late, after the expensive decisions are already made.
The stronger model is a partner with healthcare delivery depth, compliance fluency, and enough product judgment to challenge weak assumptions early. That includes teams experienced in custom healthcare software development who can discuss FHIR maturity, PHI boundaries, cloud controls, release strategy, and AI model governance in one working session.
AI is part of the reason this role has expanded. Many buyers no longer want a team that can merely integrate a model endpoint. They want an engineering partner that can determine whether the model should be used at all, what data it can safely touch, how outputs will be reviewed, and how performance drift will be handled after launch.
A healthcare project starts going off track the moment compliance, security, and workflow fit are treated as post-build clean-up.
The payoff is measurable. Product teams get clearer scope decisions. Security and compliance reviews happen earlier, with fewer late surprises. Interoperability work is scoped as core platform engineering, not an afterthought. That is why the role has changed in 2026. The right partner creates ROI through better decisions, lower rework, safer AI adoption, and systems that can survive production use in healthcare.
From Vendor to Partner: What Sets Them Apart
A healthcare vendor delivers against stated requirements. A healthcare engineering partner improves the requirements before development work starts, then shares accountability for what happens after go-live.
That difference shows up early.

On a typical healthcare program, the expensive mistakes are rarely pure coding errors. They come from weak assumptions about data ownership, unclear approval paths for PHI access, poor fit with clinical workflow, and AI features that looked promising in a demo but create review burden or risk in production. A vendor waits for those issues to surface. A partner presses on them during discovery, architecture, and release planning.
What a vendor usually does
For tightly bound work, a vendor can be the right choice. If the task is well specified, low risk, and isolated from regulated workflows, straightforward execution is often enough.
That model breaks down fast in healthcare.
A patient-facing intake flow can trigger consent questions. An interface project can expose inconsistent source data. A dashboard request can become a question about audit trails, role-based access, and record retention. By the time those issues appear in QA or security review, the team is already paying for rework.
What a strategic partner does differently
A strategic partner treats delivery as one part of the job. The rest is risk reduction, decision support, and system design that stands up under compliance review and daily operational use.
In practice, they ask sharper questions before committing to scope:
-
Workflow fit: Who uses this, at what point in care or operations, and what delay or extra click is unacceptable?
-
System ownership: Which platform is the source of truth, and what happens when two systems disagree?
-
Compliance control: What logging, access, and approval steps are required before this feature can handle PHI?
-
Operational failure: How does the product behave during downtime, bad input, or partial integration failure?
-
AI governance: Is AI appropriate here, what data can it use, and who reviews outputs when confidence is low?
Those questions change the economics of the project. Teams avoid building features that cannot pass review, cannot be adopted by clinicians, or cannot be supported safely after launch. They also find better uses for AI. In strong partnerships, AI is applied where it reduces manual effort, improves triage, or speeds documentation without weakening auditability or human oversight.
I look for one more signal. A real partner is willing to challenge the brief. If the proposed architecture increases compliance overhead, if an AI feature creates more validation work than value, or if an integration introduces brittle dependencies, they say so plainly and offer an alternative.
That is the shift from vendor to partner. The work moves from “build what we asked for” to “help us make decisions that hold up in production, in audits, and in the hands of clinical users.”
Six Core Capabilities Every Healthcare Engineering Partner Needs
Healthcare projects rarely fail because a team cannot write code. They fail because the partner cannot handle regulated data, brittle integrations, production risk, or the operational reality of clinical use. The six capabilities below separate a short-term vendor from a healthcare engineering partner that can improve delivery speed, reduce audit friction, and create room for AI and interoperability work that produces ROI.
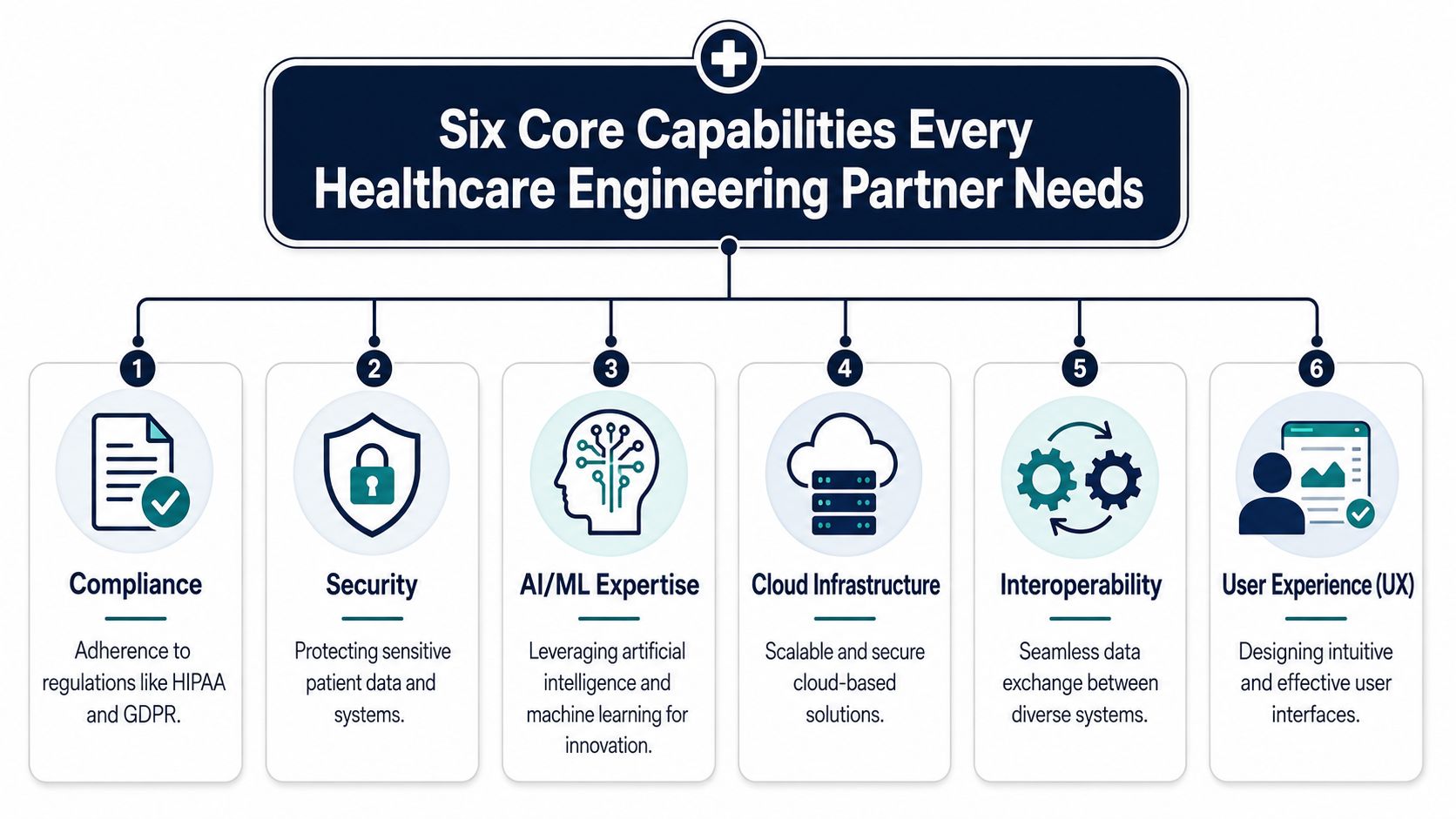
Compliance literacy
Compliance decisions shape the system long before legal review. Data classification, audit logs, access policies, retention rules, validation evidence, and release approvals all affect architecture and delivery cost.
A capable partner can explain how they document regulated engineering decisions, how they limit exposure to PHI across environments, and what evidence they produce for audits and client security reviews. If the answer stays at “HIPAA-compliant development,” keep probing. Serious teams can point to controls, approval paths, and artifacts.
Security engineering
Security work in healthcare has to be routine, not episodic. The partner should be able to walk through encryption boundaries, key and secrets management, identity design, API protection, dependency scanning, patching expectations, and incident handling in plain terms.
Security also needs to show up in delivery habits. Threat modeling before build, secure code review during implementation, and remediation windows after testing are all good signals. For teams reviewing partner capabilities, cyber compliance solutions can help frame what mature security support should cover.
AI and ML delivery discipline
Healthcare buyers often ask whether a partner can build AI. The better question is whether they can put AI into production without creating clinical, legal, or operational problems.
That means clear data boundaries, model monitoring, human review paths, output controls for generative systems, and a fallback plan when confidence is weak or source data is incomplete. It also means knowing when not to use AI. A good partner will reject AI features that add validation burden without enough workflow value. Teams assessing AI development services should look for production judgment, not just model experience.
Interoperability depth
Interoperability is where many healthcare projects lose time and budget. FHIR support alone does not prove competence. Strong teams can discuss HL7 v2 parsing, terminology mapping, canonical data models, consent-aware exchange, API versioning, and what happens when source systems send incomplete or inconsistent data.
They also test for downstream reliability, not just message acceptance. Ask how they validate mappings, reconcile source-to-target differences, and protect analytics or AI features from bad upstream data. Bridge Global’s guide to healthcare data engineering is a useful reference point for the kinds of pipeline and integration questions worth asking.
Cloud architecture and operational resilience
Cloud choices affect cost, recovery time, isolation, observability, and change risk. In healthcare, those trade-offs have to be explicit.
A mature partner can explain why a workload belongs in a managed service, container platform, or isolated environment, and what that choice means for PHI exposure, rollback, and support. They should also have a clear position on monitoring, backup validation, disaster recovery, and release controls for systems that clinicians or patients depend on. If you want to compare how partners package this work, review different full-cycle delivery service models before you commit.
Quality assurance and product usability
Healthcare QA has to cover more than feature correctness. It needs regression control, integration testing, edge conditions, data validation, permission checks, and workflow realism. Usability belongs in the same conversation because a product that is technically correct and painful to use still creates risk.
The strongest partners test with the actual context in mind. They examine handoffs between roles, error recovery, alert fatigue, and the small delays that cause clinicians to work around the system instead of using it as designed.
Here’s a practical evaluation view:
| Capability | What to ask | What weak answers sound like |
|---|---|---|
| Compliance | How do you document regulated engineering decisions? | “We follow best practices.” |
| Security | How do you handle access, audit trails, and remediation? | “Our developers are security aware.” |
| AI/ML | How do you control model output risk in production? | “We can add AI later.” |
| Interoperability | How do you test FHIR mappings and downstream consistency? | “We’ve worked with APIs before.” |
| Cloud | How do you design for rollback and resilience? | “We deploy on AWS or Azure.” |
| QA and UX | How do you validate workflow fit with real users? | “We do UAT at the end.” |
These six areas determine whether a partner can do more than ship tickets. They show whether the team can help you reduce rework, contain compliance cost, integrate AI responsibly, and build systems that survive production reality. Bridge Global is one example of a firm working across healthcare AI, data pipelines, interoperability, and secure software delivery.
Finding Your Fit: Choosing an Engagement Model
The wrong engagement model creates friction even when the engineers are strong. In healthcare, model choice affects escalation speed, stakeholder access, governance, and support continuity.

Offshore, nearshore, hybrid, and embedded
Each model can work. The question is whether it matches the risk profile of your project.
-
Offshore teams: Often fit well when the scope is stable, documentation is strong, and the internal product owner can drive decisions consistently.
-
Nearshore teams: Usually help when collaboration intensity is high and working-hour overlap matters for workshops, demos, and incident response.
-
Hybrid models: Useful when you want a blend of cost control, domain leadership, and round-the-clock execution.
-
Embedded or long-term teams: Best when the partner needs to absorb product context, compliance nuance, and operational knowledge over time.
What healthcare changes
Healthcare projects raise the bar on handoffs. A timezone gap is manageable for normal product work. It's harder when a clinical workflow issue needs same-day clarification from operations, security, and engineering. The more production-critical the platform, the more embedded the partner should feel.
A few decision filters help:
-
How often will clinical or compliance stakeholders need live access to the team?
-
Will the project require deep system discovery across legacy environments?
-
Is there an ongoing support burden after launch?
-
Do you expect architecture and product decisions, or mainly execution?
If your roadmap includes integrations, regulated data, and iterative AI features, choose an engagement model that rewards continuity, not constant re-explaining.
For organizations comparing structures, product engineering services are often more suitable than ad hoc project staffing because they align discovery, build, release, and support under one operating model.
A dedicated development team tends to work especially well when your platform is evolving over multiple phases and the same engineers need to retain architectural memory.
A Framework for Selecting Your Ideal Partner
Healthcare organizations routinely underestimate partner selection risk because standard software procurement methods miss the failure points that show up later in production. The gap usually appears in integration quality, security discipline, release control, and the partner's ability to turn AI ideas into governed clinical workflows instead of demo features.

A better selection framework tests whether the team can act as a long-term engineering partner. That means judging how they make architecture decisions, how they handle regulated delivery, and how they connect product choices to operational and financial outcomes.
Start with evidence, not claims
Case studies only help if they expose engineering decisions. Ask what systems they integrated, how they controlled access, what audit requirements shaped delivery, and what happened after go-live. Strong proof includes design trade-offs, not just polished UI screenshots.
Useful evidence usually shows up in details like these:
-
Architecture choices: Why they selected a given cloud pattern, data model, or interface strategy
-
Regulated delivery: How they documented controls, approvals, validation steps, and release readiness
-
Operational fit: How they set up monitoring, support ownership, and escalation paths
-
AI governance: How they handled human review, model risk, prompt controls, and workflow placement
If a partner cannot explain why a specific technical choice was made under healthcare constraints, expect trouble later. Teams that have done this work before can usually show that history through healthcare software delivery case studies, not generic claims about industry experience.
Ask RFP questions that expose execution maturity
A capable healthcare technology engineering partner should answer in concrete terms. Vague process language is a warning sign, especially on projects involving PHI, legacy systems, or AI-supported workflows.
Use questions that force real discussion:
-
Interoperability: How do you validate FHIR mappings, version interfaces, and catch schema drift before it breaks downstream workflows?
-
Security: What controls are required before protected data reaches development, test, or analytics environments?
-
Clinical workflow: How do you test whether the product reduces clicks, re-entry, and handoff delays for real users?
-
AI readiness: How do you choose between rules, machine learning, and generative AI for a healthcare use case?
-
Support model: Who owns incidents after launch, and how is root-cause analysis fed back into product improvement?
Good answers include examples, failure modes, and decision criteria. Weak answers stay at the level of frameworks and certifications.
Test whether they can handle AI in real care delivery
AI capability matters now, but the useful question is narrower than many RFPs suggest. The issue is not whether the partner has an AI team. The issue is whether they can build AI features that fit regulated workflows, produce traceable outputs, and stay supportable once clinical and operational teams start relying on them.
That means evaluating workflow design as seriously as model selection. A partner should be able to explain where human review sits, how output quality is monitored, what happens when confidence is low, and how the feature affects staff workload. In healthcare, measurable ROI comes from fewer manual steps, faster routing, better documentation quality, and fewer preventable support events. It does not come from adding AI labels to standard features.
Use a staged review, not a beauty contest
A short, structured process works better than a long vendor bake-off because it shows how the team thinks under pressure and how quickly they turn ambiguity into a practical plan.
| Stage | What to evaluate |
|---|---|
| Discovery call | Do they frame the business problem, constraints, and risk areas accurately? |
| Technical review | Can they reason through interoperability, security, data boundaries, and deployment realities? |
| Delivery review | Do they show a repeatable operating model with clear controls and decision ownership? |
| Team review | Are the proposed engineers and architects credible enough for regulated healthcare work? |
| Pilot or workshop | Can they turn unclear requirements into a workable roadmap, with trade-offs made explicit? |
Partners with mature AI transformation framework methods or clearly defined custom software development processes usually perform better in this stage because they can connect strategy, implementation, and governance without losing control of scope or quality.
Measuring Success KPIs and Real-World ROI
If you only measure delivery speed, you’ll miss whether the partnership improved operations. In healthcare, success shows up in workflow stability, data quality, support burden, uptime, and preventable manual effort.
That’s why KPI design should start before the build begins. A healthcare technology engineering partner should help define what success looks like in operational terms, not just project terms.
KPIs that matter more than velocity
Good measures often include:
-
Operational reliability: Fewer failures, cleaner integrations, and lower incident volume
-
Workflow performance: Less re-entry, fewer handoffs, and reduced admin burden
-
Data confidence: Better consistency across systems and fewer reconciliation issues
-
Support efficiency: Faster diagnosis and clearer ownership when something breaks
-
Adoption quality: Sustained use by clinical, operational, or patient-facing teams
In healthcare technology management, AI-enabled solutions delivered by engineering partners can drive 50-70% reductions in facility management costs, 40-60% improvements in system reliability, and USD 1.2-3.5 million in annual savings per organization through prevented equipment failures, according to Grand View Research’s healthcare technology management market report.
What ROI looks like in practice
The strongest ROI cases usually don’t come from flashy feature launches. They come from removing recurring friction and making systems easier to trust.
For example:
-
An integration modernization program: Success would be measured by fewer manual corrections, fewer escalation cycles, and cleaner downstream reporting.
-
A clinical support application: Success would depend on adoption, response time, and whether it fits actual care team behavior.
-
A maintenance or asset intelligence platform: Success would center on reliability, avoiding failures, and operational predictability.
That’s also why reviewing client cases in healthcare is useful. Not to hunt for generic success stories, but to see whether the work shows operational thinking, integration depth, and measurable business effect.
Measure what the organization gains after launch, not what the team shipped before launch.
Frequently Asked Questions about Healthtech Partners
How long should a first engagement take?
The first phase should be long enough to expose risk and define architecture, but short enough to avoid months of abstract planning. For a critical healthcare project, a focused discovery and planning phase is usually the right start. If a partner wants to jump directly into feature delivery without clarifying data flow, compliance boundaries, and integration scope, that’s a bad sign.
Who should own architecture decisions?
Your internal leadership should own the final decisions, but the partner should bring options, trade-offs, and implementation consequences clearly to the table. In regulated projects, architecture can’t be left entirely to a procurement process or a general product backlog. It needs direct involvement from engineering, security, and business owners.
How should intellectual property be handled?
Spell it out in the contract before work begins. That includes code ownership, model artifacts where applicable, documentation, deployment scripts, design assets, and any reusable components. Healthcare teams should also define ownership of integration mappings, data models, and compliance documentation, because those become business-critical very quickly.
What kind of support should exist after launch?
Post-launch support shouldn’t be vague. Define incident handling, response expectations, release ownership, monitoring responsibilities, and what counts as enhancement versus maintenance. A serious partner plans for operations early, especially when the application touches patient data or clinical workflows.
Should one partner handle both AI and core platform engineering?
Often yes, but only if they have depth in both. Splitting AI and platform work across disconnected teams creates handoff risk. Models need the right data pipelines, access controls, UI behavior, and monitoring setup to be useful in production.
What’s the simplest way to test whether a partner is right?
Run a structured workshop or small discovery engagement. Give them a real problem with real constraints. Watch how they ask questions, handle uncertainty, and identify risk. Strong partners improve your thinking before they write a line of code.
If you’re evaluating options for a complex healthtech roadmap, Bridge Global can help assess architecture, interoperability, AI readiness, and delivery model fit for your next project.
A strong Bridge Global engagement starts with the same question every healthcare leader should ask any prospective partner: can this team help us reduce risk while building something that works in the clinical and operational environment? If that’s your priority, review your shortlist against the criteria above, compare their delivery model, and ask for evidence that they can handle compliance, integration, and AI as one system rather than separate workstreams.
About Stephanie Cornelissen
Stephanie Cornelissen is a Technical Solutions Consultant with strong experience helping organizations navigate complex digital change. She works closely with teams to align business goals with practical, scalable technology solutions. With expertise in system architecture, integrations, and emerging technologies, she focuses on solving real-world problems through thoughtful execution. She enjoys working where technology meets business strategy and measurable growth.
View all posts by Stephanie Cornelissen →