


Healthcare App Development Lifecycle: A Complete Guide
Healthcare app projects rarely fail because a team cannot ship code. They fail because regulatory scope, data handling, clinical workflow, and release controls were defined too late. Typical delivery timelines still run from several months to well over a year, with meaningful time spent before launch on discovery, design, development, testing, and compliance review, as noted earlier.
That timing changes how a CTO or product leader should frame the work. In regulated software, the first hard decision is usually not technical. It is whether the product could create HIPAA exposure, trigger device classification questions, affect care decisions, or require a higher standard of validation than the team planned for.
The healthcare app development lifecycle works best as an operating model for risk reduction. Every phase should answer a practical question: what are we making safer, clearer, or easier to prove right now? That lens helps teams make better trade-offs on scope, architecture, documentation, and release pace before those choices become audit findings or production incidents.
I have seen teams lose months by treating compliance as a review step near launch. In practice, compliance changes product requirements, data boundaries, vendor selection, testing depth, and incident response expectations from the start.
That is why some organizations bring in a healthtech software development partner with experience across engineering, security, and regulated delivery. The value is not an extra process for its own sake. It is tighter decision-making across clinical, technical, and compliance constraints, with fewer late-stage surprises.
The Modern Healthcare App Lifecycle: A Framework for Risk
Traditional product teams often think in three verbs: design, build, ship. Healthcare doesn't reward that mindset. It rewards teams that can reduce uncertainty early, document decisions clearly, and prove that the software behaves safely under real operating conditions.
The modern healthcare app development lifecycle is best treated as a continuous risk-management framework. Each phase exists to prevent a different kind of failure. Discovery prevents the wrong product from being built. Architecture prevents weak security and brittle integrations. Development prevents undocumented change. Validation prevents unsafe behavior from reaching production. Monitoring prevents yesterday's compliant release from becoming tomorrow's incident.
Healthcare software succeeds when product, engineering, compliance, and operations make decisions as one system, not as separate workstreams.
That is why the process feels heavier than general SaaS delivery. It is heavier. It has to be. If the app touches protected health information, supports care delivery, or influences medical decisions, the team has to think beyond features and velocity.
A practical way to lead the work is to ask one question in every phase: what risk are we reducing right now?
| Lifecycle area | Primary risk it manages |
|---|---|
| Discovery | Building the wrong product or triggering the wrong regulatory path |
| Architecture | Security gaps, scaling limits, and integration fragility |
| Development | Uncontrolled change and weak traceability |
| Validation | Clinical usability failures and unsafe defects |
| Operations | Post-release security, reliability, and compliance drift |
Leaders who understand this usually make better trade-offs. They don't ask for speed at any cost. They ask for the fastest path to a safe, supportable product.
Phase 1: Discovery and Regulatory Strategy
A large share of healthcare product failure is set in motion before any code is shipped. The early mistakes are usually the same. Teams define features before intended use, promise integrations before confirming system access, and commit to launch dates before understanding privacy, security, and regulatory exposure.
That is why discovery in healthcare is a risk decision, not a requirements workshop.
The first job is to define what the product is allowed to do, what it must never do, and what claims the business can safely make. An app for scheduling and reminders creates one set of obligations. An app that influences triage, medication decisions, or chronic disease management creates a very different validation and regulatory burden. The distinction matters because intended use drives almost every expensive decision that follows, from data collection to testing depth to commercial positioning.
Teams entering custom healthcare software development often underestimate how quickly vague positioning turns into technical debt. If product marketing says "decision support" but the backlog was written as "patient engagement," engineering can end up building the wrong controls, QA can miss the wrong hazards, and sales can create commitments the product cannot defend in procurement or audit.
Start discovery with risk boundaries
Feature lists have value, but they are not the starting point. Start with five boundary questions:
-
What is the intended use?
This determines product claims, validation scope, and whether medical-device analysis is required.
-
What data will enter the system?
PHI, payment data, device data, and de-identified analytics data each create different control requirements.
-
Who will act on the output?
Risk changes if the user is a patient, clinician, care coordinator, or admin.
-
Which external systems are required?
EHRs, labs, pharmacies, SSO providers, and payer platforms can become schedule drivers and contract blockers.
-
What could cause harm if the product is wrong or unavailable?
That answer shapes escalation paths, logging, uptime expectations, and test planning.
I push teams to answer these questions in plain language first. If the answers only make sense to compliance counsel or architects, they are not ready to guide delivery.
Discovery outputs should reduce downstream ambiguity
A strong Phase 1 usually produces a small set of artifacts that engineering, legal, security, and clinical stakeholders can all use without reinterpretation:
-
Product requirements document with user roles, workflows, clinical touchpoints, integration assumptions, non-functional requirements, and explicit exclusions
-
Data privacy impact assessment covering collection, storage, access, sharing, retention, deletion, and cross-border concerns where relevant
-
Preliminary regulatory strategy that records intended use, claims boundaries, HIPAA obligations, consent assumptions, and whether FDA review should be analyzed
-
System context map that shows trust boundaries, user types, admin surfaces, third-party dependencies, and data flows
-
Risk register with ranked delivery and compliance risks such as EHR dependency, audit logging gaps, identity design, and clinical review bottlenecks
These are working controls. They are not slide-deck artifacts. They give architecture a stable target, help product avoid accidental scope creep, and give compliance teams something concrete to review before expensive rework begins.
The real trade-off is not speed versus process
The common mistake is treating discovery as overhead to minimize. In regulated software, weak discovery creates delay later in forms that are harder to recover from. Security controls get retrofitted after architecture decisions are already fixed. Buyer diligence requests expose missing policies and undocumented flows. Clinical reviewers raise concerns after the team has already built workflows that are unsafe or misleading.
A good discovery phase shortens the expensive parts of delivery because it removes false assumptions early.
It also sets the standard for operational discipline. Even if your delivery model is not managed services, guidance on meeting ISO 27001 compliance for MSPs is useful here because it forces clarity on control ownership, documentation, and how risks are tracked over time. That mindset matters in healthcare, where compliance is not a gate at the end. It is evidence that your team can make controlled changes without losing trust.
For teams that need a practical planning model, this digital health speed and compliance whitepaper is a useful reference before scope, budget, and release targets are locked.
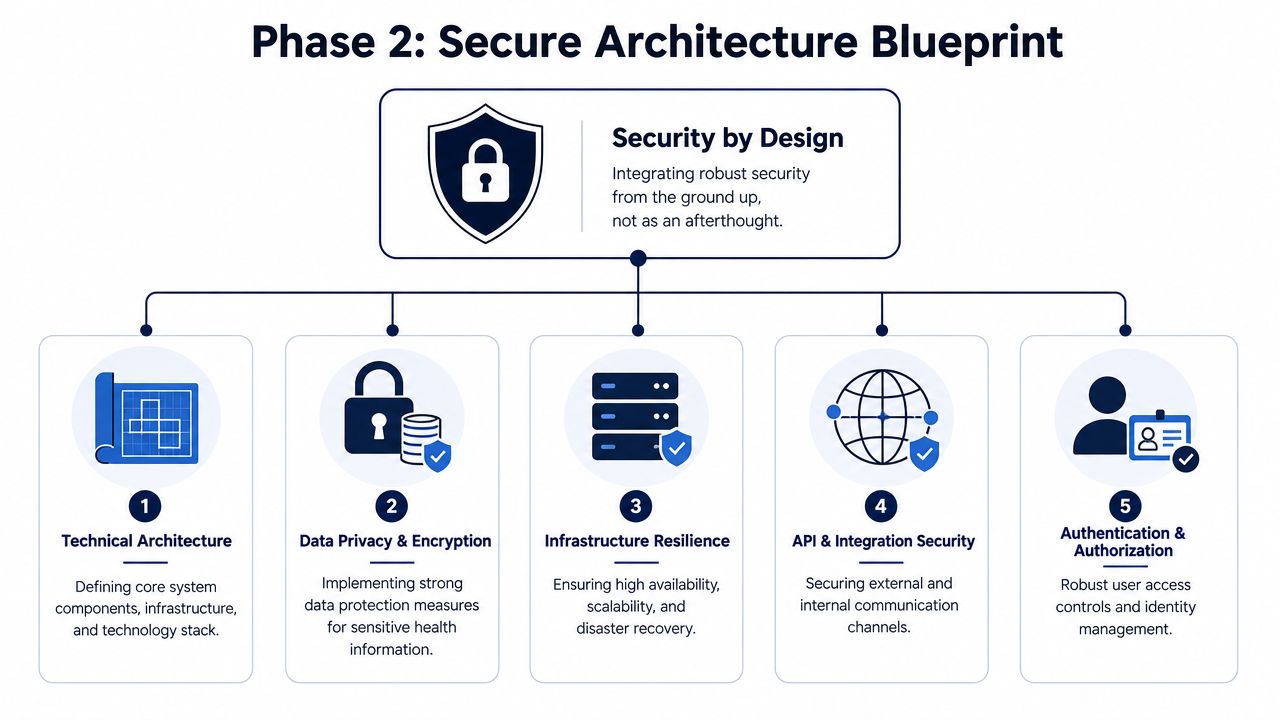
Phase 2: Architecture and Security by Design
Architecture is where healthcare software becomes expensive to fix. A weak user story can be rewritten in a sprint. A weak security model, tenancy design, or integration pattern can stay with the product for years.
Industry guidance treats healthcare app development as a multi-phase lifecycle because early stack and architecture choices shape performance, scalability, and cost over the long term. It also stresses that teams need business, clinical, technical, and regulatory alignment from the start, with agile sprints and continuous testing keeping requirements synchronized across the lifecycle, as described in this overview of healthcare app development.
Security has to exist in the blueprint
Security by design means the architecture assumes sensitive data, privileged users, and external audits from day one. It doesn't wait for a later hardening sprint.
That usually changes decisions in a few concrete ways:
-
Hosting choice matters because you'll need a cloud environment and vendor terms that support healthcare obligations, including a Business Associate Agreement where applicable.
-
Identity design has to support least-privilege access, admin separation, and verifiable role behavior.
-
Data modeling should make retention, deletion, segmentation, and de-identification feasible without heroic refactoring.
-
Auditability needs event logging at the service and workflow layers, not just infrastructure logs.
-
API posture must assume that partner systems, mobile clients, and admin tools can all become attack paths.

Interoperability is usually harder than teams expect
Plenty of healthcare products look sound in demos and fail during integration. The failure point is rarely the API call itself. It's a semantic mismatch, inconsistent patient identifiers, incomplete event handling, document variability, and vendor-specific interpretations of standards.
For that reason, planning healthcare integrations belongs in architecture, not as a post-MVP enhancement. Teams should decide early how they'll handle FHIR resources, HL7 message transformations, retry logic, reconciliation workflows, and what happens when source systems send partial or stale data.
A practical architecture review should answer questions like these:
| Question | Why it matters |
|---|---|
| What data enters from external systems? | Determines trust boundaries and validation rules |
| Where is PHI stored and replicated? | Affects encryption, retention, and access control |
| Can tenant data be cleanly isolated? | Reduces privacy and operational risk |
| What happens when an upstream EHR fails? | Protects workflow continuity and user trust |
| Are logs safe to retain and analyze? | Prevents PHI leakage through observability tooling |
If your architecture diagram doesn't show trust boundaries, it isn't a security architecture. It's a component map.
Teams often bring in specialists for threat modeling and secure design reviews at this point. That's also where dedicated cybersecurity services can help validate whether the proposed stack, access model, and deployment topology will hold up in production.
Phase 3: AI Integration and Data Governance
AI can add real value in healthcare software, but only when it solves a workflow problem that teams already understand. The worst implementation pattern is adding AI because investors expect it or because a product demo looks more modern with a chatbot panel.
The better pattern is to target one of three categories. Administrative acceleration, clinical workflow support, or operational decision assistance. Each has different governance requirements, failure modes, and validation expectations.
Choose use cases that fit the workflow
Good healthcare AI use cases tend to share one trait. They support decisions or reduce friction inside an existing workflow rather than forcing clinicians or staff to invent a new one.
Examples include summarizing intake information for care teams, structuring unformatted notes, triaging inbound messages, surfacing likely documentation gaps, or supporting risk review in care management operations. These are not trivial use cases. But they are more governable than broad claims about diagnosis or autonomous recommendations.

Data governance is the real AI product
Most healthcare AI programs don't fail because the model is weak. They fail because the surrounding controls are weak. Training data is inconsistent. Labels don't reflect clinical reality. Access to source data isn't well governed. Output behavior isn't monitored after release.
For that reason, a serious AI workstream needs clear rules for:
-
Data provenance so the team knows where training and evaluation data came from.
-
Consent and usage boundaries so the organization doesn't repurpose sensitive data casually.
-
Label quality because noisy labels create false confidence.
-
Model explainability at the level required for the product's workflow and risk profile.
-
Human review policy that defines when a clinician, operator, or support team member must validate output.
-
Change control so retraining and prompt updates are governed like product changes, not side experiments.
AI in healthcare isn't a feature sprint. It's an operating model with model governance, human oversight, and release discipline.
An AI implementation roadmap matters. It helps teams sequence data preparation, validation, user adoption, and control design instead of trying to ship a model before the organization is ready.
A capable partner can support that work across data engineering, prompt design, validation workflows, and deployment controls. Teams evaluating AI development services should ask practical questions about auditability, model monitoring, fallback behavior, and clinical review rather than just asking which model provider they use. In enterprise settings, the same discipline carries into broader enterprise AI solutions, where governance and system integration matter more than novelty.
Phase 4: Compliant Development and CI/CD
Healthcare teams don't need to choose between agile delivery and compliance. They need a development system that makes compliant behavior the default. That's the primary job of DevSecOps in a regulated product.
In practice, that means user stories carry acceptance criteria for security, logging, and traceability. Pull requests require evidence, not just approval. Build pipelines that enforce repeatable checks before code moves forward.
What an audit-ready pipeline looks like
A compliant delivery pipeline should produce a record of what changed, who approved it, what was tested, and what evidence is available if an auditor, enterprise customer, or internal reviewer asks later.
That usually includes these controls:
-
Work item traceability from requirement to commit to test evidence.
-
Automated code checks for quality, dependency issues, secrets exposure, and policy violations.
-
Security testing gates, such as static and dynamic analysis, where appropriate.
-
Environment controls so that test, staging, and production differences are limited and documented.
-
Release approvals tied to risk level, not just team preference.
-
Artifact retention for builds, test reports, and deployment records.
Agile still works, but it has sharper edges
A common mistake is treating documentation as a separate compliance stream. That creates lag, gaps, and arguments over what was tested. Strong teams generate evidence during the work itself. Test cases, threat model updates, architectural decision records, release notes, and validation artifacts are created as part of normal development.
The practical result is that compliant teams can move faster with less chaos. They aren't stopping every few months to reconstruct what happened. They already know.
For organizations building regulated products through custom software development, this operating model matters more than the exact toolchain. You can implement it with GitHub Actions, GitLab CI, Azure DevOps, Jira, TestRail, SonarQube, Snyk, or other combinations. What matters is whether the pipeline enforces discipline consistently.
One delivery option for teams that want this structure built into execution is Bridge Global's approach to AI-assisted engineering and product delivery. It combines cross-functional delivery with compliance-aware workflows, which is useful when internal teams don't yet have a mature regulated SDLC.
Phase 5: Rigorous QA and Clinical Validation
A healthcare release can pass every standard software test and still fail in practice. The gap usually shows up in edge conditions that matter in care delivery. A delayed alert, a mislabeled patient state, a permission flaw that exposes PHI, or a workflow that clinicians interpret differently under time pressure.
Quality assurance in healthcare is risk control. The goal is not only to prove that features work. It is to show that the product behaves safely, predictably, and clearly in the situations that carry the most clinical and operational consequences. Teams new to regulated delivery often underestimate this phase for the same reason they underestimate the whole lifecycle. The hard part is not writing test scripts. The hard part is proving, with evidence, that the system is fit for its intended use.
Four testing layers that need different evidence
I usually separate Phase 5 into four layers because each one answers a different risk question.
-
Functional testing asks whether units, services, integrations, and user workflows behave correctly across normal and failure conditions. In healthcare, high-risk paths deserve deeper coverage than low-risk convenience features. Medication-related actions, patient identity matching, consent handling, audit trails, and notification logic should never get the same testing depth as a profile-edit screen.
-
Performance and resilience testing ask what happens under pressure, partial failure, and recovery. Clinical operations do not fail gracefully just because the UI stays up. Background jobs can stall, queues can back up, third-party systems can throttle, and retries can create duplicates. Test plans should reflect those realities.
-
Security testing asks whether the controls you designed earlier hold up under real usage. That includes authentication flows, authorization boundaries, session behavior, API abuse paths, secret exposure, logging hygiene, and data leakage through error handling or exports.
-
Usability validation asks whether the right user can interpret the system correctly and act without avoidable confusion. This is often where serious risk appears. A screen can be technically correct and still unsafe if a care coordinator, clinician, or patient misunderstands status, urgency, or patient context.
A general app QA lifecycle reference can help structure test stages. Healthcare teams need to extend that baseline with privacy controls, safety checks, workflow realism, and role-based validation.
Clinical validation raises the standard
If the product starts approaching the Software as a Medical Device scope, QA alone does not answer the core question. The team may need clinical validation that shows the software supports its intended use and does not introduce unacceptable patient risk.
That changes who must be involved. Engineering cannot own the evidence alone. Compliance, security, product, clinical advisors, support teams, and sometimes external validation partners all have a role because each group sees a different failure mode. I have seen products clear internal QA and still break down during clinical review because the team tested feature behavior, not decision context.
In ecommerce, a defect may cost a transaction. In healthcare, the same level of defect can alter treatment context, expose PHI, or delay action by the wrong person.
The practical implication is simple. Test plans should be traceable to risk. For every high-impact workflow, the team should be able to answer three questions. What could go wrong? How would we detect it before release? What evidence shows that the residual risk is acceptable?
Published client cases can help teams compare how delivery decisions, validation depth, and domain complexity affect real projects.
Phase 6 Deployment Monitoring and Improvement
Launch is not the finish line in the healthcare app development lifecycle. It is the point where your assumptions meet production traffic, real users, partner systems, and an evolving threat environment.
A clean deployment starts with the basics done well. Hardened infrastructure. Least-privilege access. managed secrets. Safe logging. Alerting that reaches the right people. A rollback plan that has been tested. But operational maturity goes beyond deployment mechanics.
Post-release discipline is part of compliance
Healthcare products need a process for watching the system after release and deciding what to do with what they find. That includes service reliability, security signals, user-reported issues, workflow friction, and adverse operational patterns.
A practical monitoring model covers:
| Area | What the team watches |
|---|---|
| Reliability | Error rates, failed jobs, integration breakdowns, latency trends |
| Security | Suspicious access patterns, privilege misuse, dependency exposure |
| Product behavior | Abandoned workflows, repeated user confusion, support tickets |
| Data quality | Missing records, mismatched identities, reconciliation failures |
| Release impact | Whether a new deployment changed expected behavior |
Treat incidents and product learning as one loop
A lot of organizations separate engineering operations from product management too sharply. In healthcare, those loops need to inform each other. A support escalation may reveal a patient safety issue. A monitoring alert may expose a poor workflow decision. A compliance review may require a product design change.
That is why long-term ownership matters. Teams need a durable model for patching vulnerabilities, handling partner API changes, reviewing access patterns, and incorporating feedback into the next discovery cycle. Different software development service models can support that, from dedicated teams to managed support structures.
For products delivered as ongoing platforms, this looks much more like SaaS product development than a one-time implementation. The product keeps evolving. So do its obligations.
The healthiest operating model is circular. Monitoring feeds backlog decisions, backlog decisions shape architecture, and architecture shapes the next release.
If you publish this article, use a clean slug that reflects the angle. Something like /healthcare-app-development-lifecycle-risk-management-guide is more distinctive than a generic lifecycle slug, and it’s less likely to collide with an existing URL.
Healthcare App Development Lifecycle FAQ
How long does the healthcare app development lifecycle usually take?
Many healthcare apps take longer than first-time founders expect because coding is only one part of the delivery effort. A practical range is often several months to well over a year, depending on intended use, integration scope, security controls, and the level of regulatory review the product triggers.
The bigger planning mistake is treating the timeline as a linear build. In practice, discovery decisions affect architecture, architecture affects validation, and validation findings often force changes back into the backlog. Teams that plan for those loops make better schedules and avoid late-stage surprises.
What causes the biggest delays in first-time healthcare projects?
The longest delays usually come from unresolved risk, not from feature implementation. Common examples include unclear product claims, slow decisions on PHI handling, underestimated EHR or payer integrations, procurement-driven security reviews, and rework after pilot feedback.
I usually see the same pattern. A team starts with a consumer app mindset, then learns that enterprise buyers want auditability, role-based access, incident response clarity, and evidence that the delivery process is controlled. That gap expands scope fast.
Do all healthcare apps need FDA consideration?
No. FDA review depends on intended use, feature behavior, and the claims made in the product and marketing language. A scheduling or administrative tool sits in a different category from software that influences diagnosis, treatment, or disease prevention.
This is why teams should define intended use early and keep it stable. If that statement shifts halfway through the project, the regulatory path, validation burden, and release plan may shift with it.
When should security work begin?
Security work starts during discovery and gets formalized in architecture. Waiting until pre-launch usually leads to expensive fixes because identity design, encryption strategy, audit logging, environment separation, and vendor risk decisions shape the whole system.
Security also has product consequences. A weak access model can block enterprise sales. Poor auditability can create compliance friction. An immature incident process can slow approvals even if the app itself works well.
How should teams think about AI in a healthcare product?
Start with the operational risk of the decision that the model will support. AI that drafts summaries has a different review burden from AI that influences triage, coding, or care recommendations.
That changes how the team should design the feature. Data provenance, human review rules, fallback behavior, version control, monitoring for drift, and retraining approvals all need to be specified before rollout. In regulated products, AI is part of the quality system, not an isolated feature experiment.
Can agile work in a regulated healthcare environment?
Yes. Agile works well if each sprint produces working software and the evidence needed to justify it. Requirements traceability, test records, design decisions, risk updates, and approval history should be part of delivery, not postponed until release time.
Teams run into trouble when agile becomes shorthand for informal changes. In healthcare, speed comes from repeatable controls inside the workflow, not from skipping documentation and trying to reconstruct it later.
What should a CTO ask a healthcare development partner before signing?
Ask how they define intended use, classify data, set PHI boundaries, document architecture decisions, manage audit logs, validate releases, and handle post-production incidents. Ask who owns compliance artifacts, how change control works, and how clinical, legal, and security stakeholders review decisions.
Also, ask what happens when assumptions change. That answer usually reveals whether the partner understands healthcare delivery as a continuous risk-management process or as a standard app built with extra paperwork.
If you’re planning a regulated digital health product and need a delivery team that can think through architecture, compliance, AI, and long-term operations as one system, Bridge Global is one option to evaluate. Their work spans healthcare engineering, AI-enabled development, and ongoing product support, which is useful for CTOs and product leaders building beyond a prototype.
About Shreesha Chandrabose
Shreesha Chandrabose is a commerce graduate with a growing passion for content writing and digital media. With a curious mind and a creative approach, she enjoys transforming ideas into simple, relatable, and engaging narratives. She loves poetry, photography, and editing, and enjoys bringing ideas to life through words and visuals.
View all posts by Shreesha Chandrabose →