


A Guide to Electronic Health Records Integration Services
A new CTO usually sees the problem before they know what to call it. A patient arrives in the ED. The allergy list lives in one system, the recent lab result sits in another, imaging is available somewhere else, and the care team is still asking the patient to repeat medications from memory. The issue isn’t a lack of software. It’s that the software stack behaves like a collection of islands.
That’s where electronic health records integration services move from a technical nice-to-have to an operating necessity. If you’re building a healthtech platform, modernizing a provider environment, or preparing data for analytics and AI, basic connectivity won’t be enough. You need integrated data that clinicians can trust, compliance teams can audit, and engineering teams can support without constant firefighting.
Why Seamless EHR Integration Is No Longer Optional
The patient’s story is familiar because fragmented care is still common. A cardiology note may never make it cleanly into the primary care workflow. A hospital discharge summary may arrive late or in a format no downstream system can use. Staff then bridge the gaps manually, which adds delay, cost, and risk.
That’s why EHR integration can’t be treated as a side project owned only by IT. It affects patient safety, clinician efficiency, charge capture, reporting, and every handoff that depends on complete information.
How EHR integration became a core healthcare function
A major turning point came during the HITECH era. A 2022 review of EHR adoption and policy reports that approximately US$27 billion in incentives were paid to physicians and hospitals for adopting and meaningfully using EHRs. The same review notes measurable operational improvements in assessment completion, documentation of medications, vital signs, pain scores, and clinical documentation overall.
The implication for a CTO is straightforward. Once digital records became widespread, the hard problem shifted from digitization to coordination. The same review says more than 75% of office-based clinicians and 96% of hospitals use an ONC-certified EHR. In other words, the question usually isn’t whether digital records exist. It’s whether your systems can exchange and use that data reliably across care settings.
Practical rule: If clinicians still reconcile patient information by phone, fax, spreadsheet, or copy-paste, you do not have interoperability. You have digital storage.
This is also why a capable healthtech software development partner matters. Integration work touches architecture, workflow, compliance, vendor coordination, and support. Teams that underestimate that mix often end up with interfaces that technically send messages but fail in production.
The business case is broader than interfaces
The cost of disconnected systems isn’t just clinical. It shows up in rework, support tickets, duplicate entries, delayed decisions, and reporting disputes. If you want a useful non-healthcare parallel, this piece on overcoming costly operational silos captures the same pattern well. Silos create friction first, then hidden operating costs, then strategic drag.
For health systems and healthtech product teams, effective integration now sits underneath nearly everything else. Patient engagement tools need it. Revenue workflows depend on it. Analytics and AI can’t be trusted without it. That’s why electronic health records integration services have become part of the core operating model, not an optional extension.
The Language of Interoperability Core EHR Standards
A new CTO usually hears the same promise in early integration discussions: “We support HL7 and FHIR.” That answer sounds reassuring until the first go-live exposes the problem. Messages may flow, but medication lists still conflict, patient identity still needs manual review, and audit teams still cannot trace who changed what and when.
That gap matters. Connectivity gets data across a boundary. Usability determines whether clinicians can trust it, compliance teams can defend it, and product teams can build on it for analytics, automation, or AI.
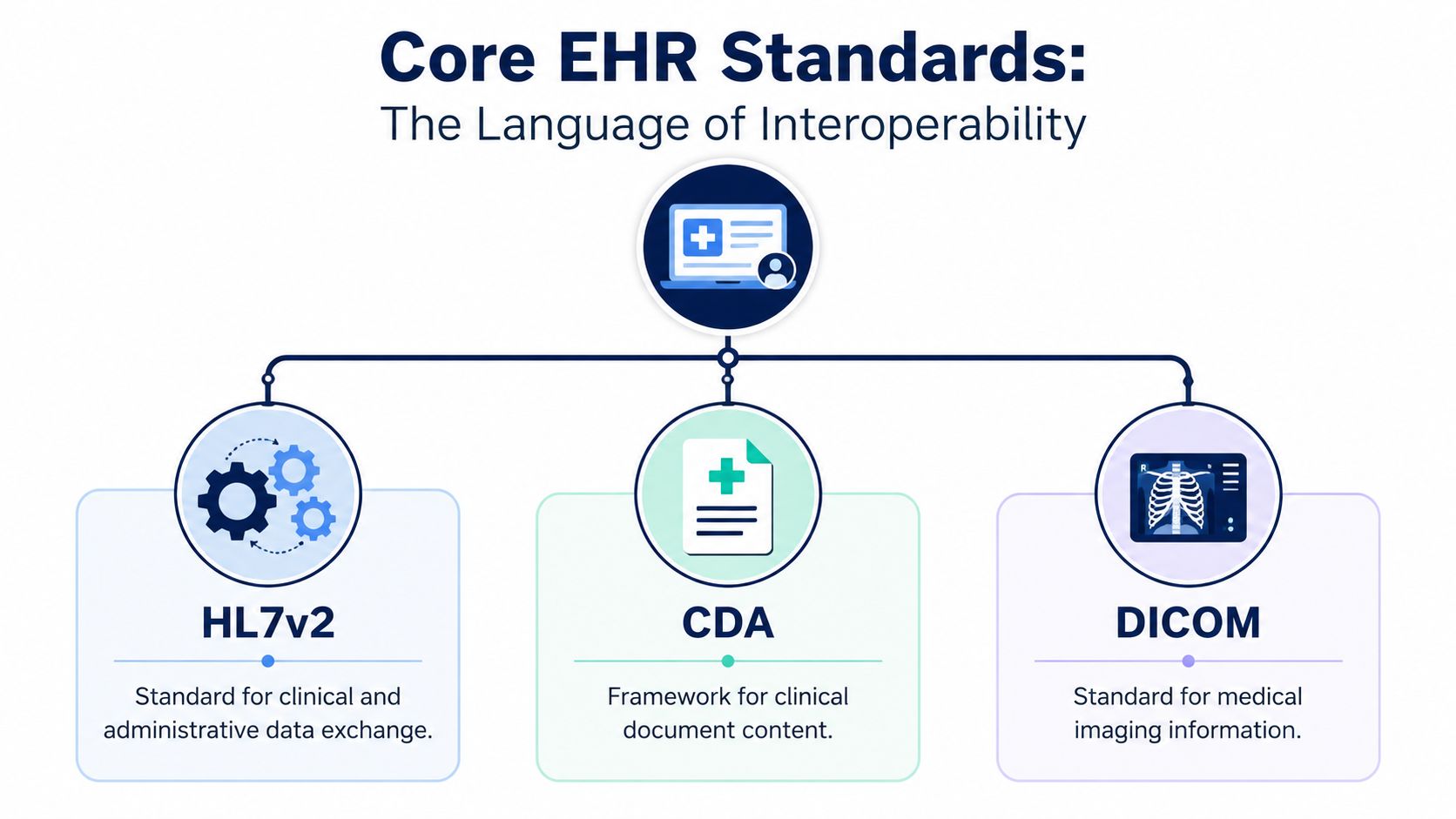
What each standard is actually for
HL7 v2 remains the operational backbone in many provider organizations. It commonly carries admissions, discharges, transfers, orders, and results. It is mature and firmly embedded in hospital operations, but implementations vary enough that interface mapping, field normalization, and exception handling still require careful engineering.
CDA handles structured clinical documents such as discharge summaries, continuity of care records, and notes. It works well when the receiving system needs a clinically meaningful document, not just a transaction payload. The trade-off is that document exchange often gives you less granular reuse of data unless you invest in parsing and normalization.
DICOM governs medical imaging and related metadata. If radiology, cardiology, or image-driven workflows are involved, DICOM is part of the architecture whether teams plan for it early or not. Imaging data brings storage, transport, viewer compatibility, and lifecycle management concerns that differ from standard clinical messaging.
FHIR defines a resource-based API model for healthcare data exchange. It is a better fit for modern applications, patient-facing products, population tools, and third-party platform integrations. It also creates false confidence when teams assume API access automatically means production-ready data quality.
Standards define syntax. They do not guarantee usable data.
As Health Catalyst notes, the ONC defines interoperability as the ability to exchange and use electronic health information without special effort by the user. That last clause is the standard worth designing around.
If a clinician still has to reconcile allergies manually across screens, your interface is active, but your interoperability is weak. If analysts cannot explain where a problem list entry came from, your data may be available, but it is not audit-ready. If an AI model consumes loosely mapped encounters or duplicated observations, the risk shifts from inconvenience to bad output and possible patient harm.
This is why teams should evaluate standards in operational terms, not just technical ones. A useful integration approach needs traceability, provenance, version handling, terminology control, and testing against real workflow conditions. For teams reviewing EHR integration tools and connectivity options, the question is not only which standard a vendor supports. Ultimately, the question is whether the resulting data can be trusted in care delivery, reporting, and downstream automation.
SMART on FHIR and CDS Hooks matter because workflow matters
SMART on FHIR lets external applications launch within the EHR with the user and patient context intact. CDS Hooks allows systems to trigger decision support at the right point in the workflow, such as medication ordering or chart review.
Those capabilities matter because clinicians do not work in standard diagrams. They work inside time-constrained workflows. Integration succeeds when the right data appears in the right context, with clear source history and access controls, without forcing staff to leave the chart and reconstruct the patient story by hand.
Comparison of Key EHR Integration Standards
| Feature | HL7 Version 2 | FHIR (Fast Healthcare Interoperability Resources) |
|---|---|---|
| Primary model | Message-based exchange | API-based resource exchange |
| Common use | Operational messaging such as ADT, orders, results | App integrations, modern data access, patient-facing and platform use cases |
| Typical environment | Legacy and mixed hospital estates | Modern web and mobile ecosystems |
| Implementation style | Interface-driven, often custom mapped | Resource-oriented, API-led |
| Strength | Mature and widely embedded in provider workflows | Better fit for reusable integrations and external applications |
| Limitation | Can be hard to normalize across implementations | Still requires workflow design, mapping, and governance |
What a CTO should listen for
“We support FHIR” is not a useful answer by itself.
Ask whether the vendor supports launch context, write-back, identity matching, terminology mapping, event subscriptions, error handling, downtime procedures, and full audit trails. Ask how they validate inbound data before it reaches clinical workflow or analytics stores. Ask how they handle inconsistent source records across sites and versions.
Standards tell you what format data can arrive in. Architecture and governance determine whether that data is trustworthy enough to use.
Architecting Connection Common EHR Integration Patterns
Most integration failures don't begin with a broken standard. They begin with a weak architecture choice that looked faster at the start. The pattern you choose affects maintenance burden, vendor dependence, scalability, and how painful every future integration becomes.
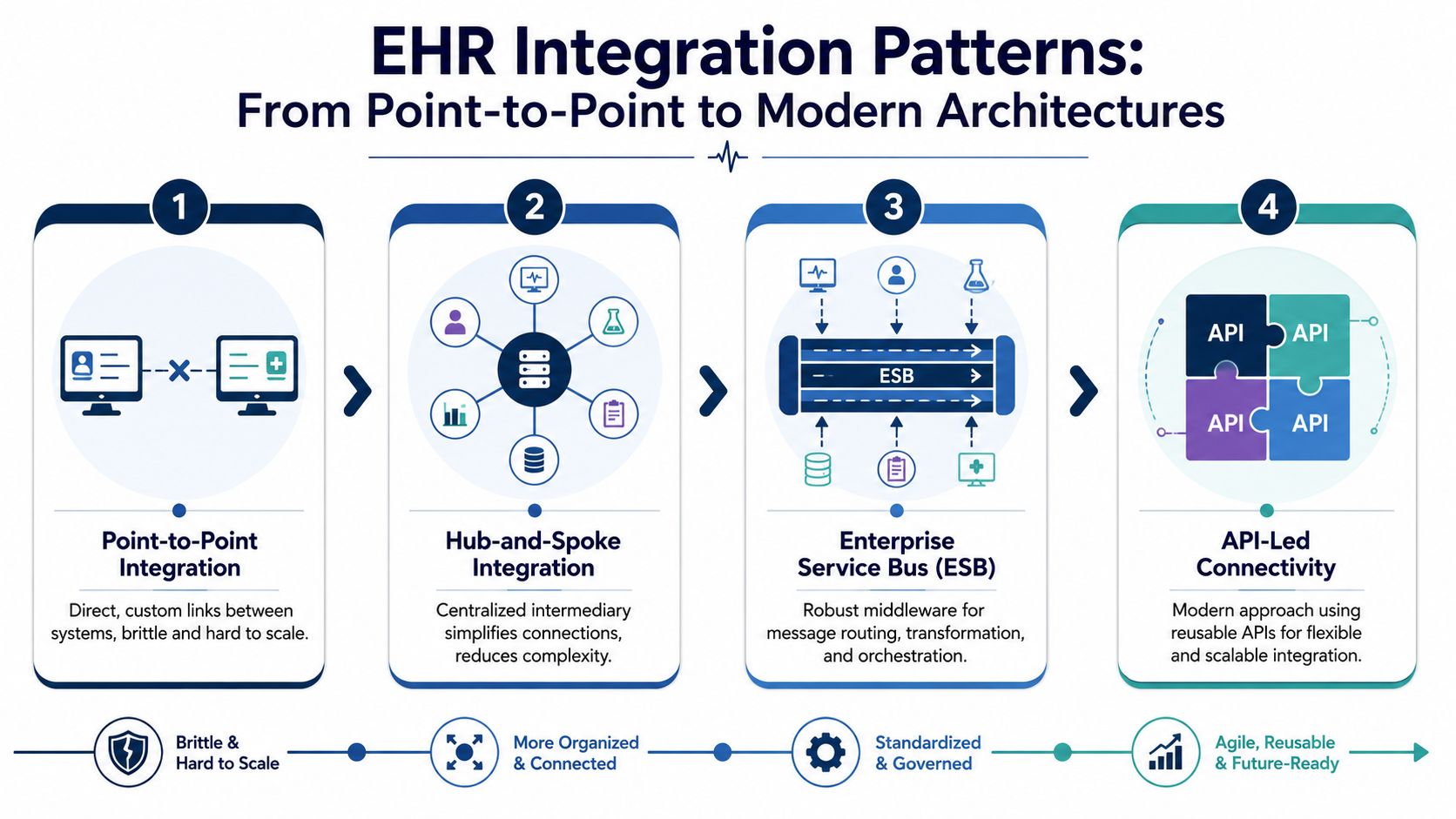
Point-to-point works until it doesn't
The simplest approach is direct system-to-system integration. One application sends to another through a custom interface. That can be acceptable for a narrow use case with stable requirements.
It becomes fragile as soon as the estate grows. Every new system adds more connection logic, more vendor-specific mapping, and more failure points. Troubleshooting also gets harder because no single integration layer owns routing, transformation, or observability.
Middleware and ESB reduce chaos, but add central dependence
A hub-and-spoke or ESB model centralizes routing and transformation. This usually improves control and reduces the combinatorial mess of point-to-point links. It also creates one place to monitor interfaces and apply common rules.
The trade-off is central complexity. If the middleware layer is badly designed, under-documented, or over-customized, it turns into a bottleneck that every team depends on and few teams fully understand.
API-led platforms fit modern product and platform teams
API gateways and interoperability platforms support more modular integration. They work well when you need reusable services, cleaner separation between systems, and better support for external apps, portals, and partner ecosystems.
For healthtech products, this pattern is often easier to scale than legacy interface sprawl. It also fits better with event-driven systems, cloud-native services, and product teams that release frequently.
Connectivity is not the main bottleneck
The hard engineering problem usually isn't opening the pipe. It's agreeing on what the data means once it arrives.
One system records a medication one way, another stores it differently, and a third buries relevant status in local custom fields. APIs may exist, but if the semantics don't align, the integrated record still won't be trustworthy.
Architect's note: Count interfaces if you want a deployment metric. Count manual corrections if you want a quality metric.
What works in mixed estates
In older provider environments, architecture should account for coexistence, not purity. That means supporting legacy HIS, LIS, RIS, patient portals, and newer apps at the same time. The goal isn't elegant diagrams. The goal is stable operations during change.
A practical pattern usually includes:
-
Canonical models where they help: Not a giant abstract data model for everything, but shared representations for high-value entities like patient, encounter, medication, and result.
-
Terminology controls: Use standardized terminologies and validation rules wherever downstream use depends on consistency.
-
Phased rollout: Start with workflows where bad integration hurts most, then expand.
-
Continuous monitoring: Validate payloads, field mappings, failures, retries, and downstream usability.
For organizations planning broader custom healthcare software development or launching products tied to SaaS product development, this architectural choice is strategic. It will shape delivery speed and support cost long after go-live. Teams comparing implementation options should also look closely at available healthcare integrations, especially if they'll be operating across multiple vendors and legacy systems.
Securing Patient Data and Ensuring Compliance
Security failures in healthcare aren't abstract governance problems. They become patient trust issues, contractual issues, and operational crises very quickly. Integration expands the attack surface because data moves across more systems, more accounts, and often more vendors.
If you want a reminder of what poor control looks like in practice, review these details of the US healthcare data breach. The lesson isn't just that breaches happen. It's that basic discipline around exposure, access, and stewardship that still breaks down.
What compliance looks like in engineering practice
For U.S. projects, HIPAA requirements should shape how you design storage, transmission, logging, and access from day one. For EU-facing systems, GDPR introduces its own obligations around lawful processing, data handling, and data subject rights. In both cases, engineering choices matter more than policy decks.
A compliant integration stack usually includes:
-
Encryption in transit and at rest: Data shouldn't move or sit unprotected.
-
Role-based access controls: Staff, vendors, and systems should only see what they need.
-
Immutable audit trails: You need to know who accessed what, changed what, and when.
-
Environment separation: Development, testing, and production need clear controls.
-
Retention and deletion policies: Integrated data shouldn't live forever just because it can.
The BAA is not paperwork theater
If a third party handles protected health information in a U.S. context, the Business Associate Agreement matters. A surprising number of teams treat the BAA as a procurement document to finish later. That's backwards.
The BAA should align with technical reality. If the vendor can access logs, backups, support tooling, or production data pathways, those responsibilities need to be reflected contractually and operationally.
Good compliance work is visible in code review, infrastructure policy, support procedures, and audit logs. If it only exists in slide decks, it won't survive an incident.
When evaluating vendors, review their secure development process, incident response approach, and auditability of changes. If security capability is a core concern, it's worth looking at specialized support such as cybersecurity services. Integration done without security rigor creates liability faster than it creates value.
A practical final check is simple. Ask whether the system can prove what happened after a disputed update, failed write-back, or unauthorized access event. If the answer is fuzzy, the compliance posture is also fuzzy.
Your Integration Roadmap and Partner Selection
A CTO usually sees the integration program after the first warning signs appear. Clinicians are reconciling mismatched records by hand. Analysts cannot trust denominator counts across systems. Product teams want AI features, but the underlying data cannot support safe inference or clean audit trails. At that point, the question is no longer whether systems can connect. The key question is whether the connected data can be trusted in production.
That is why roadmap discipline matters. Teams that skip workflow analysis, provenance rules, and post-go-live ownership often end up with interfaces that pass messages but still create operational risk.
Grand View Research's EHR market outlook estimated the global EHR market at US$35.89 billion in 2025 and projected it to reach US$53.11 billion by 2033, with a 5.10% compound annual growth rate from 2026 to 2033. The same source states that EHR integration efforts can range from US$50,000 to US$500,000+, with implementation commonly taking 3 to 9 months and extending to 12 to 18 months in complex legacy environments. Those numbers are a useful reminder. Partner selection affects not just delivery speed, but long-term support cost, compliance exposure, and patient safety.
A practical delivery roadmap
Discovery and strategy should identify more than source systems and endpoints. Map the clinical or operational decision each workflow supports, who owns the data at each step, what level of timeliness is required, and what failure looks like in real use. If the integrated output will feed analytics or machine learning later, define minimum expectations for completeness, provenance, and normalization from day one.
Architecture and design should turn those requirements into explicit rules. Choose standards and transport methods, define canonical models where needed, set patient-matching logic, and decide how the team will detect mapping drift. This is also the point to decide whether you are building for one interface or for a reusable integration layer.
Development and integration should stay narrow at first. Prove one high-value workflow end to end, with real exception handling and traceability, before expanding the scope. Teams that try to connect every system in one wave usually delay value and make defect isolation harder.
Testing and validation should answer a business question, not just a technical one. Did the medication list arrive in the right place? Did a duplicate patient record get created? Can a support engineer trace why a write-back failed? For organizations preparing data for advanced use, this is also where AI delivery capabilities for regulated product teams become relevant. Clean outputs depend on disciplined validation upstream.
Deployment and training should be staged by risk and workflow dependency. Start where support coverage is strong, user feedback is fast, and rollback is realistic. A quiet pilot with clear ownership is usually more valuable than a broad launch that overwhelms operations.
Maintenance and optimization need a named owner, a budget, and change control. EHR vendors revise fields, upgrade APIs, and alter behavior. Internal workflows also change. If nobody owns interface health after go-live, data quality degrades long before anyone opens a ticket.
Questions worth asking every potential partner
Use vendor meetings to test operating judgment.
-
How do you handle mixed standards and partial modernisation?
A credible partner should be able to work with HL7 v2, FHIR, document exchange, flat files, and older vendor constraints in the same program.
-
How do you verify data usability after transport succeeds?
Message delivery is only one checkpoint. Ask how they validate semantic accuracy, reconciliation outcomes, and downstream reporting impact.
-
What does support look like after launch?
Delivery quality depends on clear ownership, escalation design, and realistic software development service models.
-
Can the integration plan support the product roadmap?
For many healthtech companies, interfaces sit inside broader custom software development, including patient apps, care management workflows, analytics pipelines, and payer connectivity.
-
How do you manage change safely?
Ask how they test vendor upgrades, review mapping changes, and document decisions that auditors or enterprise customers may later question.
What separates a steady partner from a risky one
The strongest partners talk in specifics. They ask where patient identity breaks down, which records drive reimbursement, what latency is acceptable for each workflow, and how support teams will investigate disputes. They also understand a hard truth in EHR work. Data that is technically integrated can still be unusable for analytics, automation, or AI if provenance, normalization, and exception handling were treated as secondary concerns.
You can often see that difference in past work. Relevant client cases are useful when they show repeatable delivery patterns, ownership after launch, and evidence that the team can work inside regulated environments.
The common buying mistake is choosing based on build price alone. The higher cost usually shows up later in rework, manual reconciliation, incident response, and delayed product initiatives. A good integration partner reduces those hidden costs by designing for trustworthy data and audit-ready operations from the start.
The Bridge Global Advantage: AI-Powered Audit-Ready Integration
The integration conversation is changing. Buyers used to ask, “Can you connect these systems?” Now the sharper question is, “Can you prove the resulting data is usable, traceable, and safe enough for clinical workflows, analytics, and AI?”

Why audit-ready engineering matters
Research on EHR-based studies makes the core problem clear. A recent review of EHR data quality limitations in research and analytics highlights recurring issues such as missingness, bias, confounding, and heterogeneity, and recommends practices such as external validation, sensitivity analysis, imputation, and supplementation with other data sources. For delivery teams, that means integration alone does not make data trustworthy.
Audit-ready engineering closes that gap by building governance and validation into the delivery lifecycle. It treats provenance, completeness, and traceability as system requirements, not reporting extras added later.
Where AI helps and where it doesn't
AI can improve integration work if it's used with discipline. It can support mapping suggestions, interface test generation, anomaly detection, payload validation, and monitoring for data quality drift. It should not be treated as a substitute for clinical workflow design, terminology governance, or compliance controls.
That's where AI development services become relevant in a practical way. Used well, they accelerate repetitive engineering work and improve validation coverage. Used poorly, they just automate confusion.
One example in this space is Bridge Global, which works as a product and engineering partner across healthcare software, AI-enabled delivery, and integration-heavy environments. For teams trying to connect systems while also preparing data for advanced use, the important question isn't whether AI is present. It's whether the process produces records that can be audited and trusted.
Integrated data becomes strategically valuable only when you can explain its origin, validate its quality, and defend its use.
Organizations planning broader AI-enabled transformation should also look at how integration fits into their enterprise AI solutions and long-term execution model. If AI initiatives are fed by inconsistent records, the problem scales faster. If the data foundation is governed and testable, advanced use cases become far more realistic.
As we explored in our guide to applied AI delivery, the winning pattern isn't “add AI later.” It's designing systems so governance, interoperability, and model-readiness develop together.
Frequently Asked Questions About EHR Integration
| Question | Answer |
|---|---|
| How do you integrate with legacy hospital systems without breaking current workflows? | Start with workflow mapping, not interface coding. Older HIS, LIS, and RIS environments often support data exchange, but the operational risk comes from changing timing, identifiers, or user expectations. Phase the rollout, validate with real users, and preserve fallback procedures during early go-live. |
| What’s the most common reason EHR integration projects disappoint? | Teams confuse connectivity with usability. Messages may flow, but clinicians still can’t trust the result, or support teams can’t trace what changed. The mapping, normalization, and governance layers usually decide success. |
| Should a startup build direct EHR integrations or use a platform? | It depends on your reach and control requirements. Direct integrations can work when the number of target environments is limited and the workflow is specific. Platforms can reduce repeated effort across multiple EHRs, but you still need to inspect how they handle workflow fit, write-back, monitoring, and support. |
| How should success be measured after go-live? | Don’t stop at interface uptime. Measure whether users access complete information faster, whether manual reconciliation drops, whether audit trails are reliable, and whether downstream analytics can use the record without excessive cleanup. |
| Can integrated EHR data be used safely for AI? | It can, but only when governance is strong. Data provenance, missingness, semantic consistency, and validation matter. If the integrated record can’t be audited and explained, it’s a weak foundation for AI. |
| How do you future-proof an integration strategy? | Choose architectures and partners that can support mixed environments. Most organizations will operate legacy interfaces and modern APIs together for a long time. Future-proofing comes from modular design, observability, terminology discipline, and change management, not from assuming one standard will replace everything. |
If you’re planning electronic health records integration services and need a team that can connect architecture, compliance, and AI-readiness in one delivery model, Bridge Global is worth evaluating as a practical engineering partner.
About Stephanie Cornelissen
Stephanie Cornelissen is a Technical Solutions Consultant with strong experience helping organizations navigate complex digital change. She works closely with teams to align business goals with practical, scalable technology solutions. With expertise in system architecture, integrations, and emerging technologies, she focuses on solving real-world problems through thoughtful execution. She enjoys working where technology meets business strategy and measurable growth.
View all posts by Stephanie Cornelissen →